
Our team
Our team at the National Institute for Data Science in Health and Medicine of the Xiamen University is a cross-disciplinary group composed of people from computer science, bioinformatics, and biology. We focus on using computational methods to solve biological and clinical questions. Currently, we are working on quantitative proteomics analysis, single cell imaging and tumor microenvironment analysis, and multi-omics clinical data platform for precision medicine. More information about our group can be found at https://xmuyu.notion.site/.

Background
Advanced melanoma has a poor prognosis with a 5-year survival rate lower than 10% 1. Immunotherapies targeting immune checkpoint molecules PD-1 and CTLA-4 leverage the immune system to fight cancer, which have shown improved survival in advanced melanoma patients 2. However, only a subset of patients benefit from immunotherapy, and currently no single biomarker is sufficient for patient stratification and response prediction, presumably due to the complex mechanisms behind cancer progression and treatment resistance.
This study tries to depict a systematic landscape of the tumor microenvironments (TMEs) of melanoma patients with different response to immunotherapy. Empowered by multiplexed single cell image analysis, we identified distinct immune archetypes from both immune hot and cold tumor environments. Each archetype has a unique cellular composition that associates with different clinical responses to immunotherapy. The findings suggest that cell compositions together with their spatial relationships may help to identify patients that could benefit from immunotherapy.
What we did
Single-cell technologies have enabled extensive analysis of the TME, including cellular compositions, trajectories and cell-cell interactions. We used imaging mass cytometry (IMC), a multiplexed imaging technique to measure the levels of proteins at single-cell resolution, to analyze tumor tissues from melanoma patients receiving anti-PD-1 therapy (Figure 1).
")
What we found
We first wondered whether the cellular compositions differ in TMEs from responders (R, n = 14) and nonresponders (NR, n = 12). Comparing the cell type abundance, we found the percentages of lymphocytes were significantly higher in responders than nonresponders, but only in the invasive margin and not core tumor region. We further identified two types of myeloid cells that play different roles for immunotherapy. MC2 cells (HLA-DR-CD14+CD16−CD11C−CD11b−) tend to have pro-tumor function while MC4 cells (HLA-DRhiCD14hiCD16+CD11c+CD11b+) are more anti-tumor.
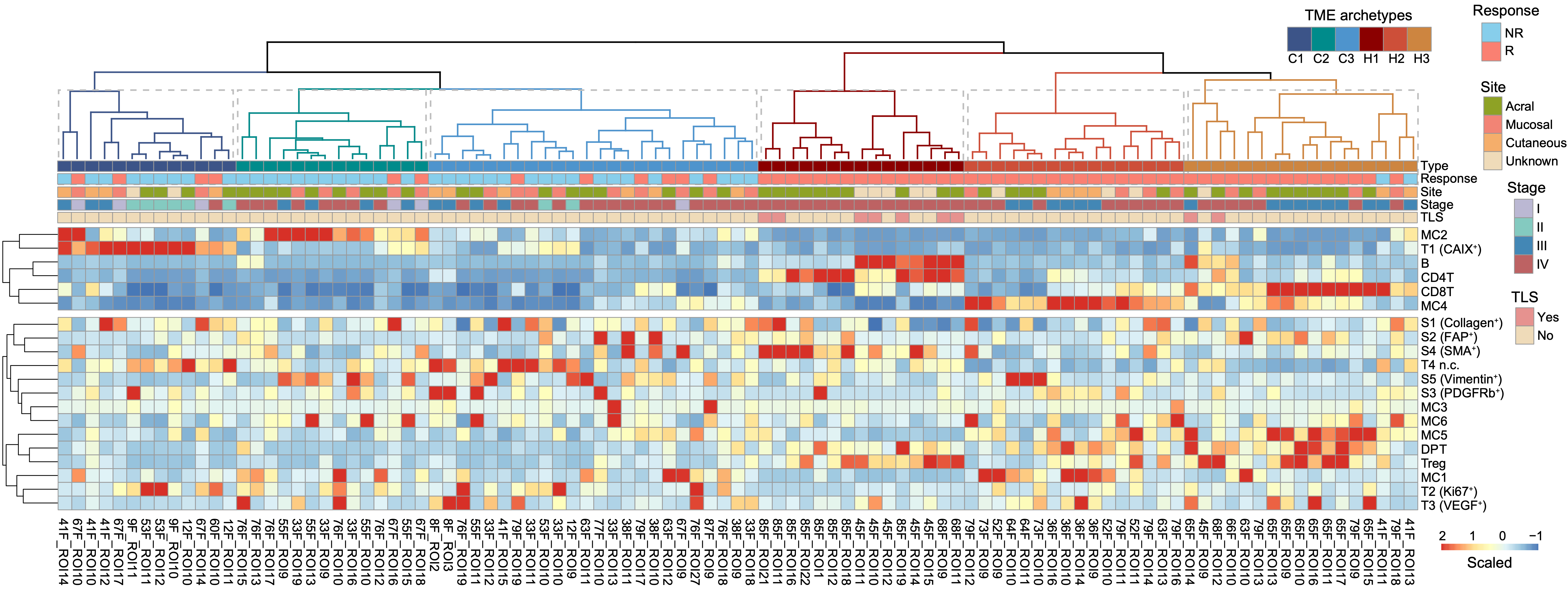
We then investigated if the cellular compositions within TMEs can separate different melanoma types and identify patients for immunotherapy. Unbiased clustering revealed six TME archetypes with distinct cell compositions, including three immune hot TMEs characterized by strong infiltration of different immune cell subtypes, including CD4+ T and B cells (H1), HLA-DR+CD11c+ myeloid derived cells (H2), and CD8+ T cells (H3), respectively, and three immune cold TMEs showing enrichment of CAIX+ tumor cells (C1), HLA-DR−CAIX+ myeloid derived cells (C2), and an archetype with no significant enrichment of any cell type (C3), respectively (Figure 2). Signal pathway analysis with bulk RNA-seq data from paired samples also identified some distinct pathways of different TME archetypes.
Based on the above classification of TMEs, we used majority voting to determine the TME type for each patient as either immune cold or hot. Kaplan-Meier analysis revealed better overall survival (OS, p = 0.0093) and progression-free survival (PFS, p = 0.06) in patients defined as immune hot, showing the prognostic performance of TME types.
What is next - Translational impact
Our results suggest that the sensitivity and resistance mechanisms of tumor to immunotherapy can be more intricate than simply immune-“hot” or “cold” TME, and demonstrate the utility of multiplex imaging technologies in studying complex molecular events in a spatially resolved manner for patient stratification strategies and treatment outcome prediction. Further investigation of each mechanism behind different TME archetypes is desired for better precision cancer therapeutics and prioritizing patients for immunotherapy.
References
1. Hodi, F. S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. New England Journal of Medicine 363, 711–723 (2010)
2. Robert, C. et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. The Lancet Oncology 20, 1239–1251 (2019)
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Jun 01, 2026
Public health and health governance in China
Publishing Model: Open Access
Deadline: Jul 31, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in