After the paper | Third generation effects of chemotherapy drug treatment?
Published in Cancer
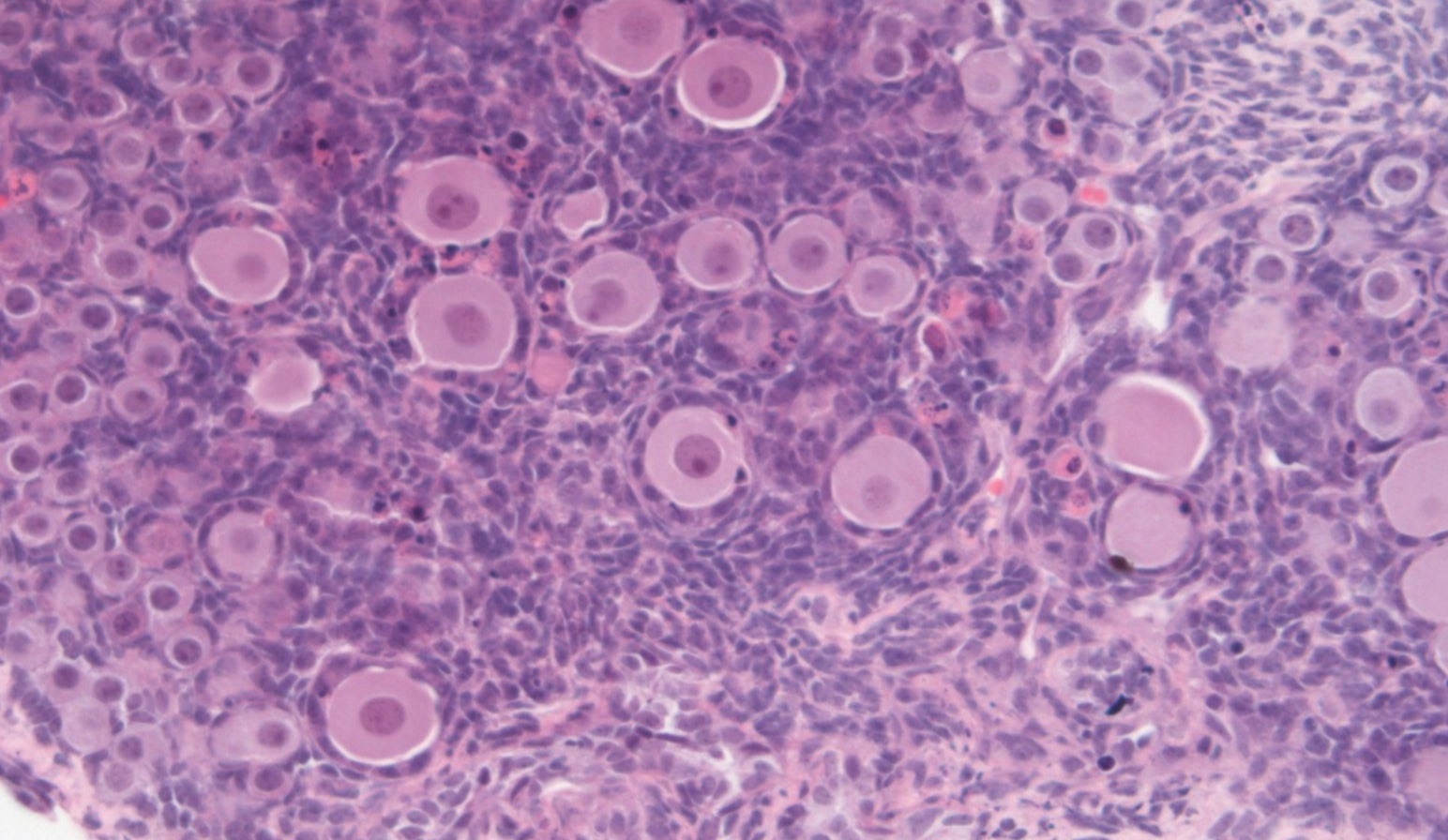

In 2016, our paper on ‘Etoposide damages female germ cells in the developing ovary’ was published in BMC Cancer. The paper explored the effects of the topoisomerase II inhibitor etoposide, a chemotherapeutic which can be given to pregnant cancer patients, on the germ cells which would be developing within any female fetus during the pregnancy. Using a mouse model, we found that etoposide damaged ovarian germ cells at very early stages, prior to formation of the ovarian follicles in which the germ cells grow and mature, but that exposure to the same, or even higher concentration of etoposide had no effect on these germ cells after the follicles had formed. This suggests that the precise timing of treating any pregnant woman with etoposide may be a crucial factor in determining the extent to which the future fertility of an exposed fetus may be affected.
So what happened after our paper was published?
AGNES
The paper received considerable attention in various news outlets (Altmetric – Etoposide damages female germ cells in the developing ovary) which I had not really expected. The reason I had initially stumbled into this area of research was something of a chance effect, as a consequence of the focus of my PhD, in which I was examining other types of topoisomerase II inhibitors, and their effect on female fertility. When I then started exploring the literature I was astonished to find that next-to-no research had been carried out to determine whether chemotherapy drugs, such as etoposide, could affect the future fertility of the exposed fetus. I was even more surprised to find out that chemotherapy treatment is considered safe to administer to pregnant women after the 1st trimester, despite the understanding that many chemotherapy agents can have damaging effects on fertility of children and young people with cancer. That discovery then lead me down this research path, since it seemed to me to be an important gap in this field. Therefore, I was delighted that the paper received so much interest in the media, since that interest would further help to highlight the gap, and explain to people why it is important for scientists and clinicians to explore this area further.
This was my first publication on which I was the first author, and I went on to present the findings from the paper at the annual Society of Reproduction and Fertility conference in 2016, winning their postdoctoral prize for that talk. This prize included a round trip to Australia to present my findings at the annual conference of the Society for the Study of Reproduction in Perth the following year, a fantastic experience, and also my first time visiting Australia.
I now have a lectureship, as part of which I am continuing to work on this topic: indeed, this has become the focus of my current research.
NORAH
I think that there are two consequences of the research project published in this BMC Cancer paper that stand out to me.
Firstly, for me this work began as part of the PhD project of my then graduate student, Agnes Stefansdottir. Agnes is the first of my PhD students with whom I have then gone on to collaborate as they have gained research independence, in this case with Agnes starting a Lectureship at the University of Edinburgh. Watching the careers of previous PhD students develop in the years after graduation is always very fulfilling, one of the highlights being a supervisor. Continuing to work with that person as has happened here, and doing so on a topic that has stemmed from that PhD project has been particularly rewarding.
Secondly, despite the fact that the need to administer chemotherapy treatment to pregnant women is, luckily, uncommon – estimates are that this will only happen in around one in a thousand pregnancies – I have been surprised to find that there have been a couple of occasions where I have met people with a personal link to this situation. Probably because the topic has not gained much general attention until recently, people caught up in this situation are particularly keen to discuss what the ramifications might be, and what it might be helpful to do. This very much brings the research topic to life, powerfully highlighting the need for the work to continue.
AGNES AND NORAH
Since the publication of our BMC Cancer paper, we have both been very pleased to see that the importance of this topic is gaining increasing recognition. One result of this is that we now have links with other scientists and with clinicians who work with pregnant cancer patients, leading to us becoming part of a collaboration of research groups across Europe.
Follow the Topic
-
BMC Cancer
This is an open access, peer-reviewed journal that considers articles on all aspects of cancer research, including the pathophysiology, prevention, diagnosis and treatment of cancers.

Related Collections
With Collections, you can get published faster and increase your visibility.
Neoadjuvant and adjuvant therapy for gynecologic malignancies
The ongoing research in this field is vital, as it contributes to improving treatment protocols and patient quality of life. Recent breakthroughs have highlighted the significance of personalized treatment approaches, such as targeted therapies and immunotherapies, which have shown promising results in clinical trials. By exploring the optimal sequencing of neoadjuvant and adjuvant therapies, researchers can provide insights into downstaging tumors, minimizing toxicity, and maximizing the overall effectiveness of treatments, leading to better patient outcomes.
Continued exploration and innovation in neoadjuvant and adjuvant therapies hold the potential to transform the management of gynecologic malignancies. Future research may focus on refining treatment regimens, identifying biomarkers for response, and integrating multidisciplinary approaches to optimize surgical and therapeutic outcomes. As we deepen our understanding of tumor heterogeneity and resistance mechanisms, new therapeutic strategies may emerge, offering hope for improved prognosis in patients with these challenging cancers.
- Efficacy of neoadjuvant and adjuvant chemotherapy
- Role of radiation therapy in treatment protocols
- Impact of neoadjuvant vs. adjuvant approaches on fertility and quality of life
- Strategies for downstaging tumors
- Integration of novel therapies in surgical planning
- Resistance mechanisms and strategies for overcoming them
- Role of molecular profiling in guiding therapy
- Clinical trials landscape and future directions
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jul 21, 2026
Prehabilitation in cancer
Prehabilitation in cancer care is an emerging field focused on optimizing patients' physical and psychological well-being prior to undergoing surgery or treatment. By incorporating strategies such as exercise, nutritional support, and psychological interventions, prehabilitation aims to enhance patients’ resilience and overall health outcomes. The concept has gained traction as healthcare professionals recognize the significance of preparing patients for the demands of cancer treatment and recovery, ultimately aiming to improve surgical outcomes and quality of life.
The importance of integrating prehabilitation into cancer care has been underscored by recent advances in research demonstrating its potential benefits. Studies have shown that tailored exercise programs and nutritional interventions can significantly improve treatment outcomes, reduce complications, and enhance recovery times. As healthcare systems increasingly prioritize patient-centered approaches, the implementation of prehabilitation practices may lead to more effective cancer management and improve the overall experience for patients navigating their cancer journey.
Continued research in this area has the potential to revolutionize cancer care practices, paving the way for the development of standardized prehabilitation protocols tailored to individual patient needs. This research may also inspire innovations in telehealth and digital health solutions that facilitate remote prehabilitation interventions, making these essential services more accessible to patients regardless of their geographical location.
Topics welcome to this Collection include, but are not limited to, the following:
- Impact of prehabilitation on surgical outcomes
- Exercise interventions in cancer care
- Nutritional support during prehabilitation
- Prehabilitation and chemotherapy outcomes
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jan 20, 2027




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in