Beyond “Wear and Tear”: The Story Behind Our Paper on Osteoarthritis Phenotypes
For decades, osteoarthritis (OA) was described rather simplistically as a “wear-and-tear” disease — an inevitable consequence of ageing joints. Yet, in daily clinical practice, that explanation never fully matched what we observed. Two patients with similar X-rays often experienced entirely different symptoms. Some progressed rapidly toward joint replacement, while others remained relatively stable for years. Some had severe pain with minimal structural damage, whereas others with advanced degeneration surprisingly reported little discomfort. These inconsistencies gradually led us to question whether osteoarthritis was truly a single disease at all.
This paper, “Osteoarthritis phenotypes: advancing precision medicine through clinical, structural, and molecular stratification,” published in International Orthopaedics, emerged from that clinical curiosity and scientific frustration.
The idea for this review emerged from numerous multidisciplinary discussions among orthopaedic surgeons, rheumatologists, imaging specialists, and genomics researchers at Indraprastha Apollo Hospitals. As clinicians, we repeatedly encountered patients who did not fit neatly into conventional treatment algorithms. Why did anti-inflammatory therapies help some OA patients but fail in others? Why did obesity influence hand OA, a non-weight-bearing joint? Why did certain patients continue to experience disabling pain even after a technically successful total knee arthroplasty (TKA)?
The answers increasingly pointed toward heterogeneity.
Over the past decade, advances in molecular biology, MRI imaging, genomics, biomarker science, and artificial intelligence have transformed our understanding of OA. We now recognize that osteoarthritis is not merely cartilage degeneration. It is a complex whole-joint disorder involving cartilage, subchondral bone, synovium, ligaments, periarticular muscles, inflammatory mediators, metabolic pathways, and even neural pain sensitization mechanisms.
While preparing this review, we realized that the field had reached a pivotal transition point. The conversation was no longer simply about osteoarthritis severity, but about osteoarthritis phenotypes, endotypes, and eventually theratypes — identifying which subgroup of patients is likely to respond to a particular treatment. Precision medicine, which has already transformed oncology and respiratory medicine, is gradually entering the world of osteoarthritis.
One of the most fascinating aspects of the writing process was appreciating the diversity of OA phenotypes.
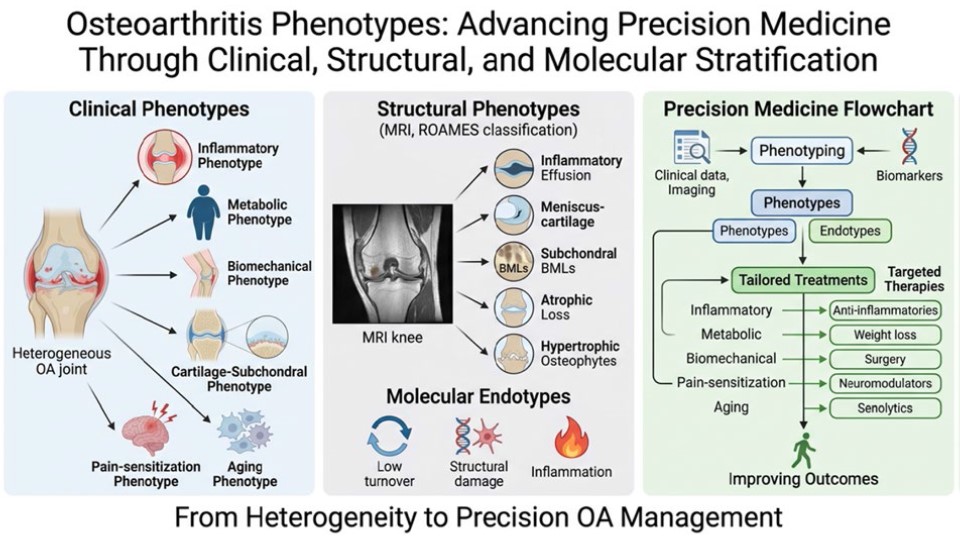
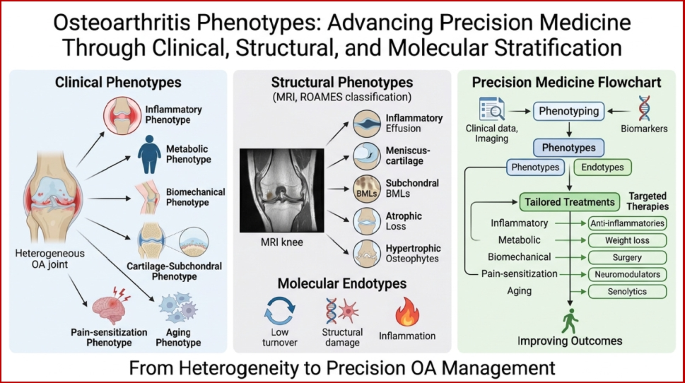
The inflammatory phenotype resembles a low-grade immunological disease characterised by synovitis, cytokine activation, and elevated systemic inflammatory markers. The metabolic phenotype links obesity, insulin resistance, adipokines, and systemic inflammation with joint degeneration. The biomechanical phenotype is driven by malalignment, instability, or meniscal injury. The cartilage–subchondral bone phenotype highlights the osteochondral unit as an integrated biological structure rather than isolated cartilage wear. Meanwhile, the pain-sensitization phenotype explains why some patients experience disproportionate pain despite limited radiographic disease. Finally, the ageing/senescence phenotype introduces the intriguing role of cellular ageing and senolytic therapies in OA progression.
As orthopaedic surgeons, we found the pain-sensitization phenotype particularly thought-provoking. Traditional orthopaedics often emphasizes structural correction — alignment, reconstruction, or replacement. Yet patients with central sensitization may continue to experience persistent pain despite technically excellent surgery. Understanding this disconnect between structure and pain may fundamentally improve patient selection and counselling before joint replacement surgery.
Another important motivation behind this work was the growing role of imaging and AI in redefining OA. Modern MRI-based classifications, such as ROAMES, now allow structural phenotyping with remarkable detail. Simultaneously, AI-assisted MRI scoring and machine-learning clustering approaches are beginning to identify patterns invisible to the human eye. Our own interest in advanced imaging, including PET-MRI and AI-based musculoskeletal imaging research, strongly influenced this aspect of the review.
The genomics revolution added another exciting layer. During the preparation of this manuscript, landmark genomic studies involving nearly two million individuals identified hundreds of OA-associated genetic loci. These discoveries reinforce that OA is not a uniform degenerative condition but a biologically diverse disease with joint-specific genetic signatures. Hip OA, knee OA, and hand OA may differ substantially at the molecular level.
One challenge we faced while writing the paper was balancing optimism with realism.
Phenotype-based OA management is conceptually appealing, but clinical translation remains incomplete. Many phenotype-driven trials have produced inconsistent or disappointing results. Anti-cytokine therapies, bisphosphonates, and several proposed disease-modifying osteoarthritis drugs (DMOADs) have not yet achieved the transformative impact many hoped for. Biomarkers remain insufficiently standardized, phenotypes frequently overlap, and most frameworks are still heavily knee-centric.
We felt it was important not to oversell precision medicine prematurely. Instead, we wanted this review to honestly reflect both the promise and the current limitations of the field.
One of the most rewarding parts of the project was developing the proposed “Integrated Clinical–Structural–Molecular Phenotyping Framework.” This conceptual model attempts to bridge the gap between research-oriented phenotyping and real-world clinical decision-making. Rather than viewing OA through a single lens, the framework integrates clinical features, imaging phenotypes, molecular biomarkers, and pain sensitization assessment into a unified approach.
Importantly, this work was deeply collaborative. Orthopaedics, rheumatology, genomics, radiology, and data science increasingly intersect in modern OA research. This review reflects that multidisciplinary spirit. The involvement of colleagues with expertise ranging from clinical rheumatology to genomics enriched the manuscript enormously and reinforced the paper's central message: OA can no longer be understood from a single-speciality perspective.
At a broader level, the story behind this paper is really about a paradigm shift.
Medicine is moving away from broad disease labels toward biologically defined subgroups. OA is following that trajectory. The future may involve identifying an individual patient’s dominant disease driver — inflammatory, metabolic, biomechanical, senescent, or sensitization-related — and tailoring therapy accordingly. Some patients may benefit most from weight reduction and metabolic optimization, others from anti-inflammatory biologics, others from biomechanical correction, and still others from neuromodulatory or senolytic approaches.
The “one-size-fits-all” era in OA management is slowly giving way to a more nuanced and personalized future.
Whether this transformation fully succeeds will depend on robust biomarkers, standardized phenotyping systems, accessible imaging technologies, and large phenotype-enriched clinical trials. But the direction of travel is becoming increasingly clear.
For us, this review was not simply an academic exercise. It was an attempt to synthesize where the field currently stands, acknowledge its uncertainties, and contribute to an evolving conversation about the future of osteoarthritis care. Most importantly, it reflects a growing recognition that behind every “OA patient” lies a biologically unique disease process — one that deserves individualized understanding and treatment.
Follow the Topic
-
International Orthopaedics
International Orthopaedics, the Official Journal of the Société Internationale de Chirurgie Orthopédique et de Traumatologie publishes original papers from all over the world. The articles deal with clinical orthopaedic surgery or basic research directly connected with orthopaedic surgery.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in
Osteoarthritis is one of the oldest diseases known to humankind, yet we do not know much about it!. It is a heterogeneous disease with several subtypes, requiring different treatment approaches.