Bridging the Data Gap for AI in Oral Cancer Detection: The MeMoSA-30000 Dataset
Published in Cancer, Research Data, and Computational Sciences

The unmet need
Oral cancer remains a major health burden in Asia, where a large proportion of global cases occur, accounting for around two-thirds of the global incidence and about three-quarters of the global mortality for the disease [1]. Many oral cancers develop from visible lesions in the oral mucosa, meaning that early detection through screening could significantly improve outcomes [2]. Yet in many regions, limited access to specialists means that lesions suspicious to be malignant are often diagnosed late [3].
Our work began in East Malaysia where, in rural or remote communities, geographic barriers further limit access to care. Some villages required hours of travel along dirt roads or by boat to reach a dental clinic. Yet even in these settings, we found that mobile connectivity was often available.
This contrast led to a simple idea: Could mobile technology be used to bridge the gap in access to oral cancer screening?

Figure 1. Geographic access barriers to oral healthcare in East Malaysia. Many rural and remote communities are separated from dental services by long travel distances, difficult terrain, and reliance on river or road transport, highlighting the challenges of accessing timely oral cancer screening.
Extending screening beyond the clinic
From this idea, MeMoSA® (Mobile Mouth Screening Anywhere) was developed as a teleconsultation tool. The aim was to enable lay healthcare volunteers and, in some cases, patients themselves to capture oral images using mobile phones and share them with clinicians for remote assessment. Promisingly, we found that teleconsultation using mobile images could achieve high diagnostic accuracy, supporting its use as a viable approach for remote oral lesion assessment [4].
MeMoSA® was piloted in community screening programmes in rural Sarawak, East Malaysia. Trained healthcare volunteers conducted screening in villages, capturing images and facilitating remote review by dentists and dental specialists.
This approach helped extend the reach of screening services beyond conventional methods. It also facilitated access to screening, as screening could be conducted in familiar environments, by trusted community members. Importantly, we found that this model was acceptable and feasible, both for the communities being screened, and for the volunteers and healthcare providers delivering the programme [5].

Figure 2. Oral cancer screening conducted in a community setting in East Malaysia. Trained healthcare volunteers use mobile devices to capture images of the oral cavity, enabling remote review by dentists and specialists.
Anticipating the next challenge
While improving access was a key goal, we also recognised that improving screening access could introduce new challenges. In particular, increasing screening coverage would inevitably lead to higher volumes of images requiring clinical review and triage.
As screening coverage increased, this anticipated issue became evident in practice. The success of teleconsultation-based community screening meant that more images, and more potential cases, were being generated. Dentists now had to review and triage a growing volume of submissions, deciding which cases required referral and which could be safely monitored.
This created a bottleneck. While MeMoSA® had improved access to screening, it also placed additional demands on already limited clinical resources, particularly at the primary care level.
Where AI could play a role
This challenge pointed to the next step: the use of artificial intelligence (AI) to support clinical workflows.
AI has shown promising diagnostic performance for detection using clinical images [6], indicating its potential to assist in identifying high-risk lesions, prioritising cases for review, and reducing unnecessary referrals. In doing so, it could help make community-based screening programmes more scalable and sustainable.
However, progress in this area has been limited by a fundamental challenge: the lack of large, well-curated datasets of oral lesion images [7].
Building the MeMoSA dataset through regional collaboration
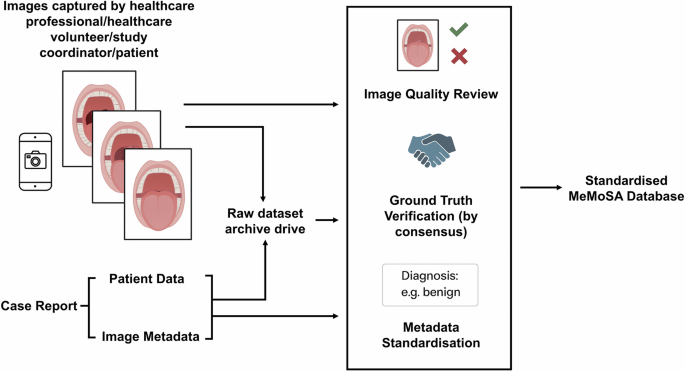
To address this gap, we developed the MeMoSA-30000 dataset: a large collection of oral mucosa images supplemented with clinical information and expert diagnoses.
Importantly, the dataset was designed not only to support AI development for lesion detection, but also to address the anticipated need for scalable triage solutions within high-volume screening programmes.
The dataset was built over nearly a decade through contributions across multiple countries, including Malaysia, India, Indonesia, Sri Lanka, and Nepal. Many of these collaborators are part of the Asia-Pacific Oral Cancer Network (APOCNET), a network supporting research partnerships in oral cancer across the Asia-Pacific region [8]. Images were captured using mobile phones by dentists, healthcare volunteers, study coordinators, and sometimes patients themselves.

Figure 3. Members of the Asia-Pacific Oral Cancer Network (APOCNET) at a stakeholder meeting, representing regional collaboration in oral cancer research and data sharing.
Importantly, a substantial proportion of the images were derived from real-world screening programmes, including those conducted in East Malaysia. This means that the dataset captures not only a wide range of lesion types, but also the variability in image quality, acquisition settings, and patient populations encountered in practice. This diversity allows the dataset to support the development of AI systems that are robust to real-world variability, an important consideration for tools intended for deployment in low-resource and community settings.
Beyond collecting images, substantial effort went into harmonising diagnostic labels, verifying clinical annotations, and ensuring image quality across sites. The result is a dataset of more than 30,000 oral cavity images, representing a diverse range of lesions and sociodemographic contexts.
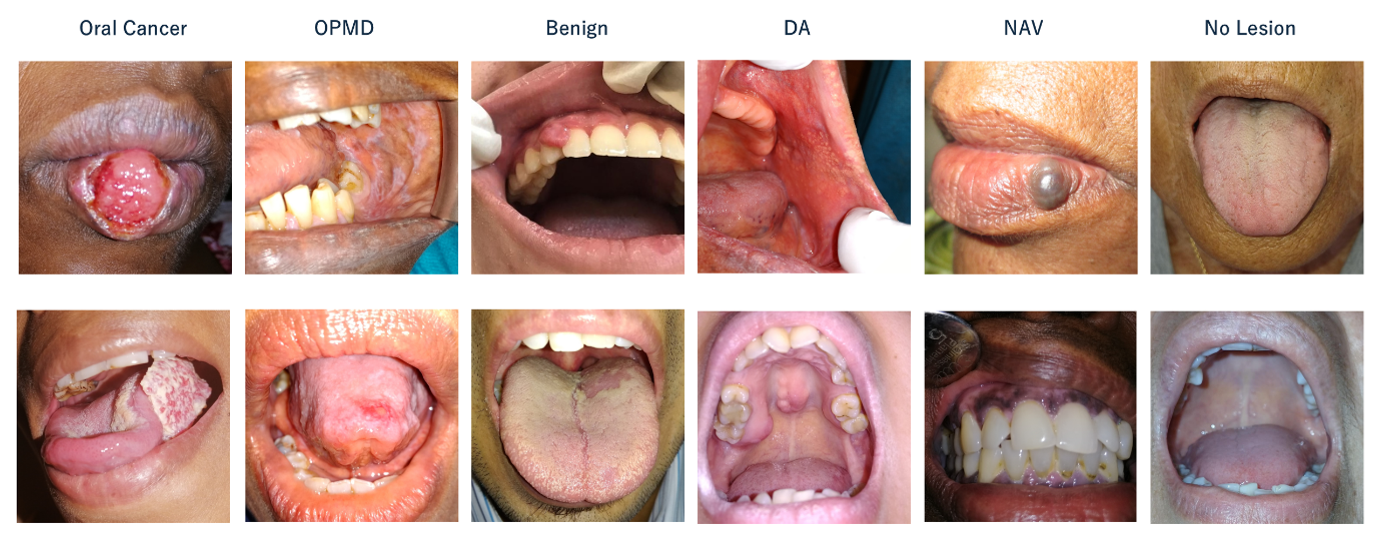
Figure 4. Example images illustrating the range of oral lesion types included in the MeMoSA-30000 dataset. Abbreviations: OPMD = Oral Potentially Malignant Disorders; DA = Developmental Anomalies; NAV = Normal Anatomic Variants.
A resource for future research
The MeMoSA-30000 dataset is available through the MeMoSA Workbench (workbench.memosa.my), where researchers can explore and access the images and associated metadata.
By making this resource available, we hope to support the development and evaluation of AI tools for oral cancer screening, particularly in settings where access to care is limited. More broadly, this work reflects an ongoing effort to move from improving access, to addressing system-level barriers, and ultimately to building scalable solutions for early detection.
References
- Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 74, 229–263 (2024).
- Sankaranarayanan, R. et al. Effect of screening on oral cancer mortality in Kerala, India: A cluster-randomised controlled trial. Lancet 365, 1927–1933 (2005).
- Nagao, T. & Warnakulasuriya, S. Screening for oral cancer: Future prospects, research and policy development for Asia. Oral Oncol 105, 104632 (2020).
- Haron, N. et al. High referral accuracy for oral cancers and oral potentially malignant disorders using telemedicine. Oral Dis 29, 380–389 (2023).
- Rajendran, S. et al. Implementation of an mHealth Oral Cancer Community Screening Program in Low- and Middle-Income Countries (LMICs): Findings from a Real-World Implementation Study. Under Review.
- Al-Rawi, N. et al. The Effectiveness of Artificial Intelligence in Detection of Oral Cancer. Int Dent J 72, 436–447 (2022).
- Sengupta, N., Sarode, S. C., Sarode, G. S. & Ghone, U. Scarcity of publicly available oral cancer image datasets for machine learning research. Oral Oncol 126, 105737 (2022).
- Sobri, S. N. S. M., Kanapathy, J., Liew, C. S. & Cheong, S. C. The establishment of the Asia-Pacific Oral Cancer Network—Inaugural stakeholders' meeting. Oral Dis 26, 1094–1097 (2020).
Follow the Topic
-
Scientific Data
A peer-reviewed, open-access journal for descriptions of datasets, and research that advances the sharing and reuse of scientific data.

Related Collections
With Collections, you can get published faster and increase your visibility.
Computer vision in plant science and agriculture
Publishing Model: Open Access
Deadline: Oct 10, 2026
Wearable and Computer Vision Data for Health and Behaviour Research
Publishing Model: Open Access
Deadline: Aug 08, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in