Can Electronic Frailty Scores Transform Chemotherapy Decision-Making? Insights from a Large UK Study
Published in Cancer
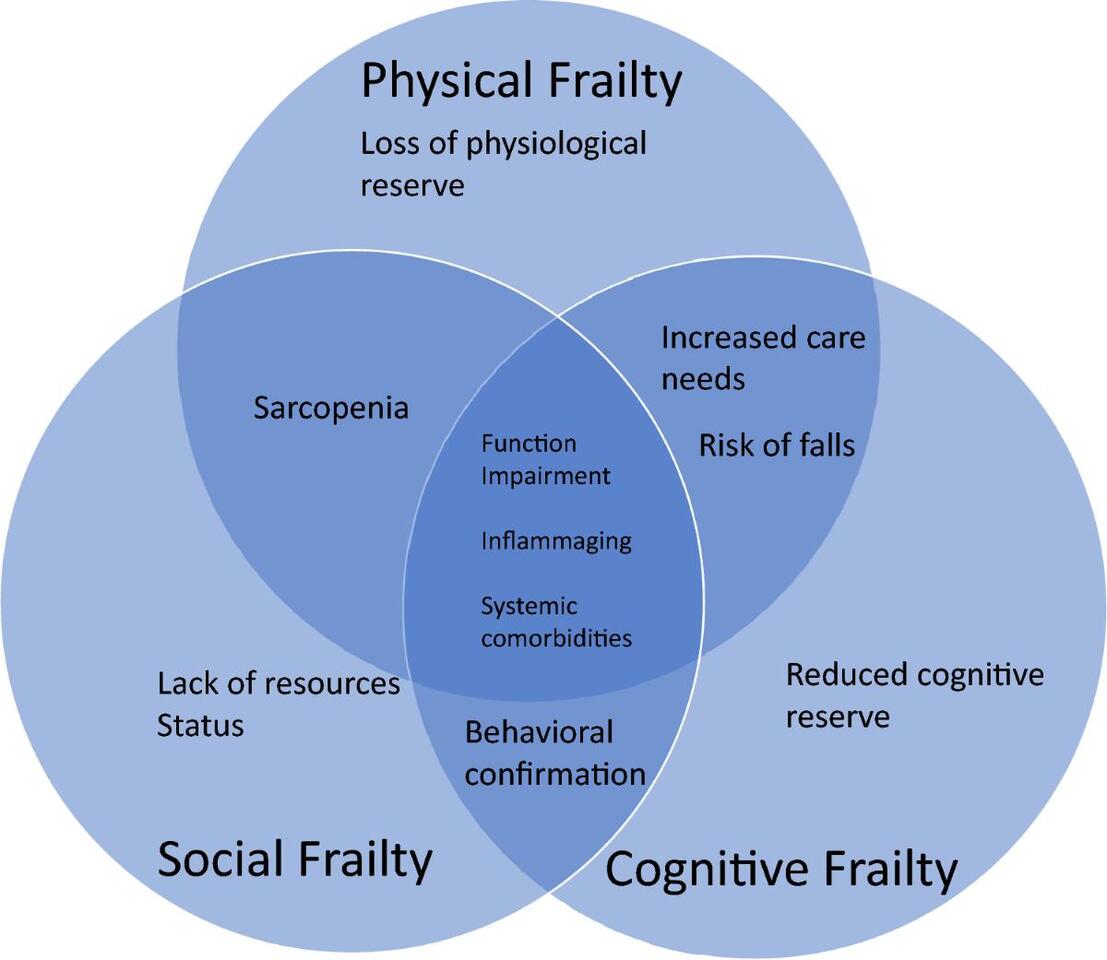
Why Frailty Matters in Oncology
Frailty is more than age. It reflects a patient’s overall vulnerability, shaped by comorbidities, functional decline, and physiological reserve. In oncology, frailty is strongly associated with:
- Increased treatment toxicity
- Higher risk of hospitalisation
- Reduced survival
Yet, frailty assessment is often inconsistent. Clinicians typically rely on performance status (PS) scores, which are quick but limited—and frequently missing in real-world datasets .
This is where automated tools like the SCARF index come in.
Drawing on data from nearly 79,000 cancer patients undergoing chemotherapy, this research highlights both the promise and limitations of electronic frailty indices in predicting outcomes such as survival and early mortality.
What Is the SCARF Index?
The SCARF index is a hospital-based adaptation of the electronic frailty index (eFI). It uses routine healthcare data to quantify frailty based on accumulated deficits.
The index incorporates 35–36 deficits, including:
- Chronic diseases (e.g. heart failure, diabetes)
- Functional limitations (mobility, falls)
- Cognitive and sensory impairments
- Social vulnerability (full list in the study)
Study Overview: A National-Scale Analysis
The study analysed chemotherapy records from England (2015–2018), including Colorectal cancer (stage III), Breast cancer (stage II–III) Lung cancer (stage IIIB–IV)
In total:
- 78,799 patients were included
- 26% were aged ≥70 years
- ~30% were classified as frail
Frailty and Survival: A Clear Gradient
One of the most striking findings is the stepwise relationship between frailty and survival.
Overall survival worsens with increasing frailty:
Fig. 1: Figure representing the risk of poor overall survival for patients ≥70 y.o. comparing to ≤69 y.o. according to the SCARF index.
From: The utility of electronic frailty index in cancer patients undergoing chemotherapy
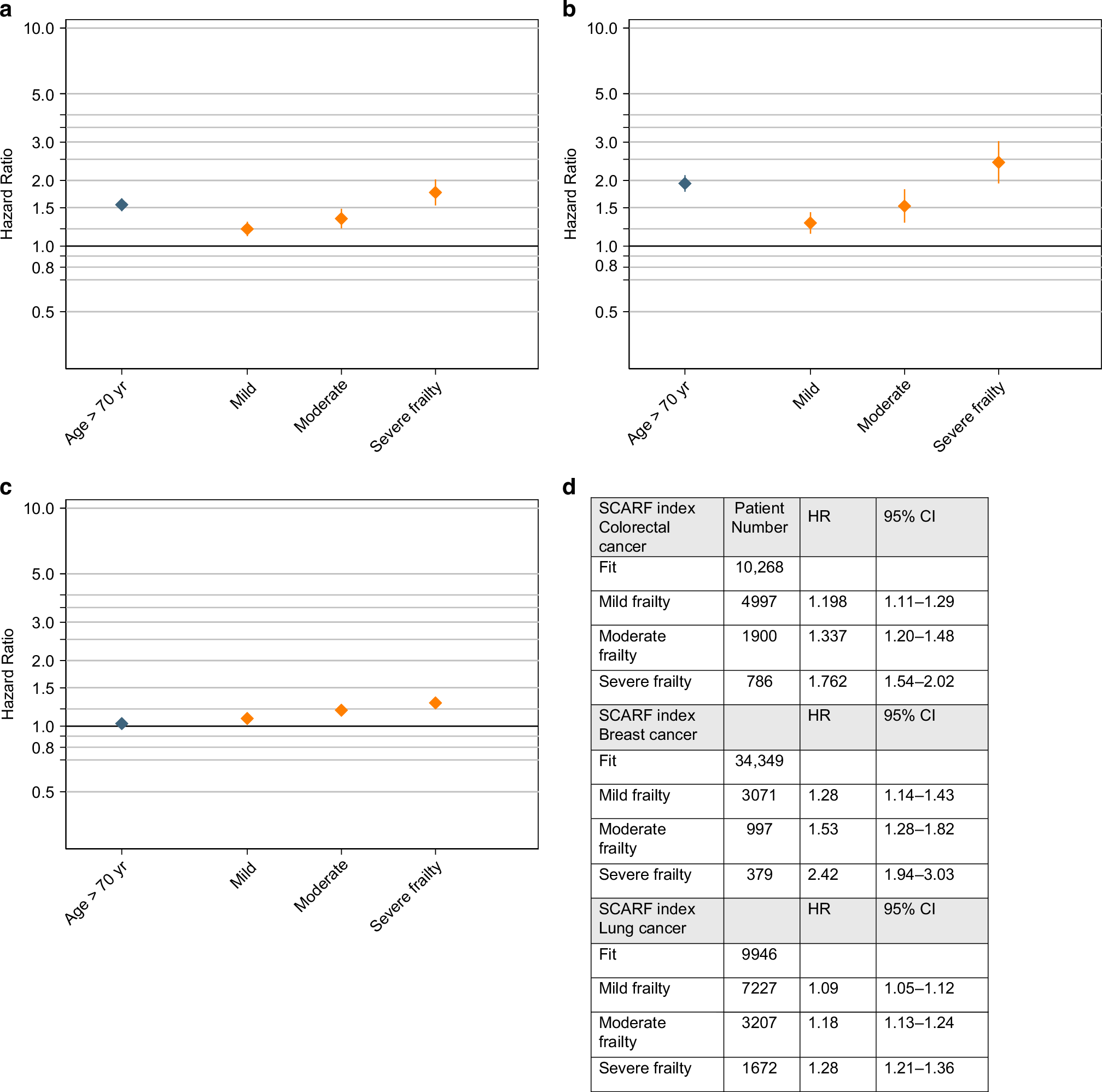
Figure A shows hazard ratio for patients with colorectal cancer, Figure B breast cancer and Figure C lung cancer. Figure D shows the numerical values for HR and 95% CI values for OS.
How Does SCARF Compare to Performance Status?
Performance status (PS) remains the standard clinical tool—but this study reveals important limitations:
- Missing data: Up to 15% of PS scores were not recorded
- Subjectivity: PS varies between clinicians
- Narrow scope: Does not capture comorbidities or long-term health
By contrast, SCARF uses objective, routinely collected data, captures multimorbidity and frailty complexity , requires no additional clinic time
However, PS still showed strong predictive power, and the two measures may be complementary rather than competing.
Implications for Clinical Practice
This study points to a future where frailty assessment is embedded into digital workflows.
Potential benefits:
- Better risk stratification before chemotherapy
- More informed discussions with patients
- Targeted referral for geriatric assessment
- Improved treatment individualisation
Because SCARF can be automatically generated from electronic records, it is particularly suited to:
- Busy oncology clinics
- Remote consultations
- Large-scale health systems
Conclusion
This large UK study demonstrates that the SCARF index is a powerful predictor of chemotherapy outcomes, particularly in breast and colorectal cancer.
While not a replacement for clinical assessment, it offers a scalable, data-driven way to quantify frailty—one that aligns with the increasing digitisation of healthcare.
For researchers and clinicians alike, the message is clear:
Frailty is measurable, actionable, and essential—and digital tools like SCARF may help bring it into routine oncology practice

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in