Designing a PKP2 Gene Therapy to Target Cardiomyocytes for Treatment of Arrhythmogenic Right Ventricular Cardiomyopathy
Published in Bioengineering & Biotechnology, General & Internal Medicine, and Pharmacy & Pharmacology

Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a life-altering cardiac disease primarily affecting active young adults with a mean age of presentation < 40 years old. The leading genetic cause of ARVC is mutation of genes encoding components of desmosomes – adhesive intercellular connections that play a critical role in ensuring proper structural anchoring and subcellular organization of cardiac muscle cells (cardiomyocytes) and electrical signaling to regulate contraction. About 40% of ARVC cases are attributable to mutations in Plakophilin-2 (PKP2) which primarily result in haploinsufficiency of PKP2 protein and disrupted desmosomes.
ARVC is a progressive form of cardiomyopathy that initially presents with syncope and/or dangerous ventricular arrhythmias, which can result in sudden cardiac arrest.(1) In fact, sudden cardiac death is the first recognized symptom of disease in nearly one in four patients.(2) As fibrofatty tissue replaces myocytes, ARVC often progresses to heart failure requiring heart transplant. Patients are strongly encouraged to limit physical exertion and stress, including participation in sports and other activities, to avoid triggering arrhythmias and hastening disease progression. Insertion of an implantable cardioverter-defibrillator (ICD) is advised, along with other standard-of-care medications for arrhythmia and heart failure. These lifestyle modifications and drugs, along with living with an ICD, negatively impact the patients’ quality of life without effectively correcting their disease state. In fact, there are no current therapies that directly address the underlying genetic cause of the disease or halt or reverse symptoms and disease progression for ARVC.
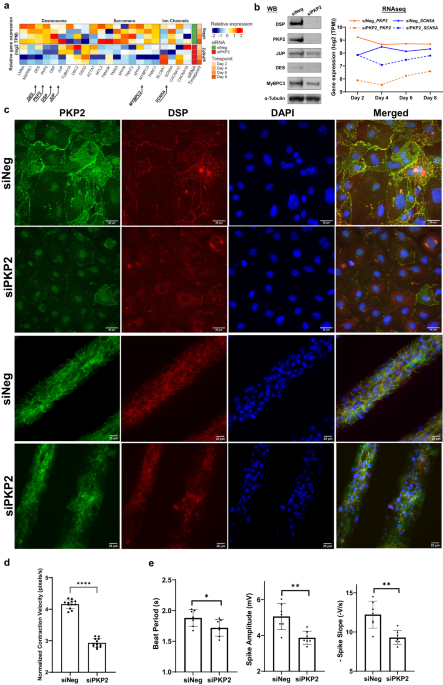
Tenaya Therapeutics is developing TN-401, a PKP2 gene therapy, intended for the treatment of patients with ARVC due to mutations in the PKP2 gene that lead to reduced PKP2 gene and protein expression. As demonstrated by Wu et al., TN-401 restores PKP2 gene and protein expression levels and function in the desmosomes of cardiomyocytes to target the underlying genetic cause of the disease. Thus, TN-401 has the potential to slow and even reverse the progression of the disease in patients with ARVC due to PKP2 mutations.
Before conducting the preclinical studies described in Wu et al., Tenaya carefully considered the optimal design of an adeno-associated virus (AAV)-based PKP2 gene therapy to target cardiac muscle via a one-time intravenous dose. There are a variety of known AAV serotypes, defined by variations in the AAV capsid sequence, each with tropism for a different subset of cell types, which can also vary depending on the species targeted. Because the gene therapy is to be delivered systemically, it was important to select an AAV with tropism for cardiomyocytes, the target cell type, and to restrict PKP2 transgene expression to this cell type using a cardiomyocyte-selective promoter. Here, we take the reader “behind the paper” to describe our selection of promoter and capsid when designing TN-401.
The ideal promoter would drive high level, selective expression in the target cell type, cardiomyocytes, while also being small enough to fit into an AAV along with the transgene payload, other regulatory elements, and the inverted terminal repeats required for AAV packaging, transduction, and formation of stable episomes, without exceeding the AAV packaging capacity of ~4.7 kb. Fortunately, such a promoter has been identified upstream of the Troponin-T2 (TNNT2) gene. TNNT2 encodes a structural protein, cardiac troponin T, which is found solely in cardiac muscle as part of sarcomeres, which are the basic unit of muscle contraction and are abundantly present in cardiac muscle. As such, it is one of the most highly expressed genes in human cardiomyocytes.(3) A 600 bp promoter has been defined that confers this high level, selective expression.(4) The small size of this promoter allows packaging in AAV along with the other elements of the PKP2 expression cassette.
Fortunately for ARVC patients, two additional sponsors are also developing PKP2 gene therapies for ARVC. Both have recently published preclinical studies on which the design and selection of their gene therapies were based.(5), (6) Both demonstrated efficacy and tolerability in mouse models of ARVC. and both also used the TNNT2 promoter to drive expression of their PKP2 gene therapy. Thus, all three PKP2 gene therapies are using cardiac-selective promoters derived from the TNNT2 gene to drive high-level expression in cardiomyocytes.
Along with the promoter, the other major element of an AAV-based gene therapy responsible for targeting the gene therapy to the cell type of interest is the AAV capsid itself. Tenaya is advancing TN-401 to clinic in the AAV9 serotype based on robust validation from multiple preclinical efficacy reports and clinical and commercial utilization for the delivery of gene therapy. Tenaya has conducted carefully controlled head-to-head studies of reporter gene delivery using a variety of leading AAV serotypes in mice and non-human primates, each concluding that, although other serotypes can target the heart, AAV9 leads the way in delivering transgene payload specifically to cardiomyocytes.
Efficacy with AAV9-based PKP2 gene therapy has been demonstrated simultaneously by three different lab groups in three different PKP2-associated ARVC mouse models. As described in Wu et al., Tenaya showed AAV9-based PKP2 gene therapy effectively prevented disease development before overt cardiomyopathy and attenuated disease progression after overt cardiomyopathy in a Pkp2 cardiac knockout mouse model of ARVC, Pkp2-cKO. Kyriakopoulou et al. showed that treatment with AAV9-based PKP2 gene therapy prevented cardiac dysfunction in an alternate ARVC mouse model, Pkp2c.1755delA/WT.(7) This model is based on a human mutation causing ARVC that was also modeled by these authors in human induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs). In a separate report, Bradford et al. also published efficacy of AAV9-based PKP2 gene therapy in yet another mouse model of ARVC carrying a Pkp2 mutation based on an orthologous ARVC-causing human mutation that affects RNA splicing.(6) In the homozygous state, this mouse model shows ARVC disease phenotypes including arrhythmias, reduced cardiac function, cardiac dilation, fibrosis, and even fat deposition in the heart – a feature of human ARVC that is not recapitulated in other Pkp2-deficient mouse models. In all three sets of published experiments, using AAV9 to deliver PKP2 resulted in prevention of disease upon early administration or a partial rescue of ARVC phenotypes with late-stage administration.
Clinically, AAV9 has the most well-established safety record of any capsid, having been dosed in more than 3000 patients worldwide with many examples of over eight years of clinical follow-up in the case of the approved SMN gene therapy for spinal muscular atrophy, Zolgensma, from Novartis.(8) AAV9 is also the only capsid with validated durable clinical transduction and gene expression in the human heart, based on data from Rocket Pharmaceutical’s LAMP2 gene therapy for Danon Disease.(9)
The selection of AAV9 was also supported by head-to-head studies of various AAV serotypes conducted by Tenaya in mice. To specifically compare the levels of cardiomyocyte expression mediated by different AAV serotypes at the same dose level, a barcoded reporter gene construct under control of the cardiomyocyte selective TNNT2 promoter was packaged into a variety of AAV serotypes, pooled, and delivered systemically to mice. Three weeks after dosing, animals were euthanized, and levels of viral genome DNA and viral transgene RNA were measured from cardiac samples (Fig. 1). Results in the left panel show that viral genome DNA load of AAV9, AAVrh.10, and AAVrh.74, after being normalized based on their representation in the pooled virus prep, are comparable, indicating that these serotypes targeted the heart equivalently. In contrast, the panel on the right shows that viral transgene RNA levels were considerably higher from AAV9 compared to AAVrh.74 or AAVrh.10. This disparity between DNA transduction in the heart and RNA expression in cardiomyocytes can be explained by the fact that the heart is composed of multiple cell types, and a readout of viral genome levels measures the aggregate transduction of all cardiac cell types, whereas a readout of RNA expression from a cardiomyocyte-specific reporter measures only effective transduction and expression in the cell type of interest – cardiomyocytes. Other studies have used a ubiquitous promoter to drive expression of a reporter gene and then measured cardiac RNA levels. In that case, the result is an aggregate of expression in all cardiac cell types and does not reflect capsid performance in terms of specifically mediating cardiomyocyte expression.
Figure 1:

Tenaya received clearance from the FDA to initiate its first-in-human RIDGETM-1 Phase 1b clinical trial of the AAV9-based PKP2 gene therapy, TN-401, in patients with PKP2-associated ARVC, and expects to begin patient dosing in the second half of 2024. The Phase 1b study will initially study a dose of 3e13 vg/kg, a level that achieved near maximal efficacy in our preclinical studies detailed in Wu et al. First-in-human trials of PKP2 gene therapies developed in AAVrh.74 and AAVrh.10 are also reported to be initiating. The advancement of multiple PKP2 gene therapies will be advantageous for ARVC patients, who stand to benefit from an effective PKP2 gene therapy with the potential to normalize PKP2 levels and desmosome function and thereby prevent, halt or even reverse the steady progression of ARVC caused by PKP2 mutations. It will also be informative for the field of cardiac gene therapy, as these multiple clinical programs will provide insights into the relative performance of different AAV serotypes in the heart, adding to our knowledge base regarding the translation of preclinical data to human experience.
References
- Basso, et al. Arrhythmogenic right ventricular cardiomyopathy. Circulation: Arrythmia and Electrophysiology. 2012;5:1233–1246.
- Dalal, et al. Arrhythmogenic right ventricular dysplasia: A United States Experience. Circulation. 2005 Dec 20;112(25):3823-32.
- Litviñuková, et al. Cells of the adult human heart. Nature. 588, 466–472 (2020)
- Mar. et al. Analysis of the upstream regions governing expression of the chicken cardiac troponin T gene in embryonic cardiac and skeletal muscle cells. J Cell Bio. (1988) 107 (2): 573–585
- Opbergen, et al. AAV-mediated delivery of Plakophilin-2a arrests progression of arrhythmogenic right ventricular cardiomyopathy in murine hearts: preclinical evidence supporting gene therapy in humans. Circulation: Genomic and Precision Medicine. 2024;17
- Bradford, et. Al. Plakophilin 2 gene therapy prevents and rescues arrhythmogenic right ventricular cardiomyopathy in a mouse model harboring patient genetics. Nat Cardiovasc Res. 2, 1246–1261 (2023)
- Kyriakopoulou, et al. Therapeutic efficacy of AAV-mediated restoration of PKP2 in arrhythmogenic cardiomyopathy. Nat Cardiovasc Res 2, 1262–1276 (2023)
- Novartis, March 4, 2024 press release
- Greenberg, et al. Danon Disease: RPO-A501 Phase 1 Results. American Society of Gene and Cell Therapy 2023
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Jun 01, 2026
Public health and health governance in China
Publishing Model: Open Access
Deadline: Jul 31, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in