Increased risk of testicular seminoma among patients with neurodevelopmental disorders
Published in Cancer
Testicular cancer is the most common cancer in young men. The incidence increases in Europe and several other parts of the world(1, 2). Ninety-five percent of all testicular cancers are testicular germ cell tumors (TGCT), of which 55-60% are seminomas and 40-45% non-seminomas(3). The underlying causes of testicular cancer are still largely unknown, but there are indications that the first steps of TGCT oncogenesis occur in utero. Some risk factors are known, such as urogenital malformations like cryptorchidism and hypospadias. Both cryptorchidism and hypospadias have been shown to be associated with neurodevelopmental disorders(4, 5). The prognosis of TGCT is currently excellent, but some individuals present with a widely disseminated disease, requiring extensive treatment to be cured(3).
The aim of this study was to investigate if history of any neurodevelopmental or other psychiatric disorder is associated with increased risk of TGCT and increased mortality.
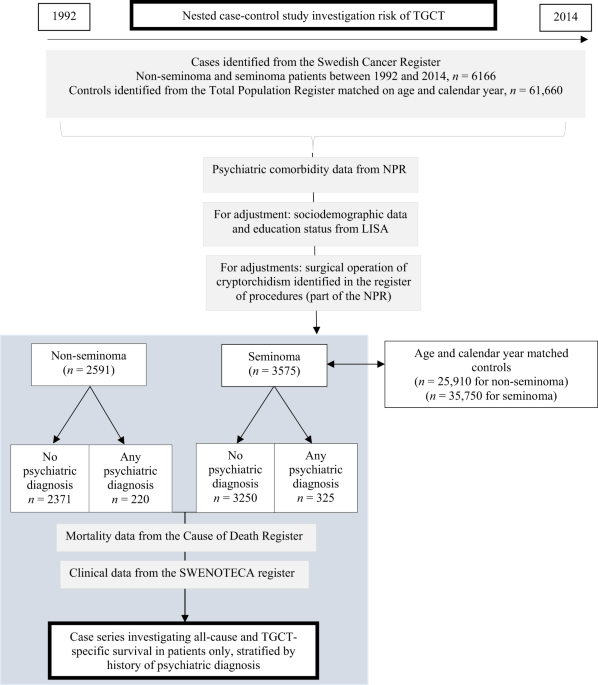
We conducted a nested-case control study including all patients diagnosed with TGCT in Sweden during the years 1992-2014, individually matched for age and calendar period of diagnosis with ten cancer-free controls each. Cases were identified from the Swedish Cancer Register and controls were identified from the Total Population Register. Mortality data were retrieved from The Swedish Cause of Death Register. Data on history of psychiatric diagnoses were retrieved from the nationwide Swedish Patient Register. Details of clinical stage were identified from the Swedish Testicular Cancer Register, held by the SWENOTECA-group. We calculated odds ratios (ORs) for the association between type of psychiatric diagnoses and TGCT risk. Among the cases, we used a cohort design and calculated hazard ratios (HRs) of the association between psychiatric disorders and all-cause and TGCT-specific mortality.
A total of 6,166 TGCT patients were included in the study, of whom 2,591 were diagnosed with non-seminoma and 3,575 with seminoma, and 61,660 matched controls. No association was found between history of psychiatric disorders and risk of TGCT overall. However, history of a neurodevelopmental disorder was associated with an increased risk of seminoma (OR 1.54; 95% CI 1.09-2.19). Since our results between neurodevelopmental disorders and seminoma remained when adjusted for cryptorchidism and congenital malformations, this could indicate that there are other possible shared risk factors than these, or a shared susceptibility between TGCT and neurodevelopmental disorders. Furthermore, seminoma patients with neurodevelopmental disorders were diagnosed at an earlier age (34 versus 38 years, p=0.004) and had more stage IV disease (5.4% versus 1.2%) at diagnosis than seminoma patients without history of psychiatric disorders. This could potentially indicate an earlier penetrance of the disease in these patients.
 In addition, in comparison to patients without psychiatric comorbidity, both the all-cause mortality and the TGCT-specific mortality were increased for patients with history of psychiatric disorders and this persisted when adjusted for age, index year, education and for cancer stage (HR 2.91; 95% CI 2.11-4.02 and HR 1.79; 95% CI 1.04-3.08, respectively) (Figure 1).
In addition, in comparison to patients without psychiatric comorbidity, both the all-cause mortality and the TGCT-specific mortality were increased for patients with history of psychiatric disorders and this persisted when adjusted for age, index year, education and for cancer stage (HR 2.91; 95% CI 2.11-4.02 and HR 1.79; 95% CI 1.04-3.08, respectively) (Figure 1).
To our knowledge, this is the first study that has investigated and observed an association between neurodevelopmental disorders and testicular seminoma. Even though the absolute risk increase was low, the results are intriguing in terms of attempts to get closer to explaining the mechanisms of testicular cancer occurrence. However, as the difference in risk was relatively small, we cannot exclude the possibility that this finding was due to chance. Hence, our finding would have to be replicated in other studies in order to be confirmed.
Furthermore, we found a worse TGCT prognosis among patients with history of psychiatric disorders. This is important to keep in mind, suggesting that one may need to be extra observant in providing these patients with the same opportunities to being successively treated, cured and followed for their TGCT.
Key findings:
- History of a neurodevelopmental disorder is associated with a 1.5 times increased risk of seminoma OR 1.54; 1.09-2.19*, p=0.015
- Seminoma patients with neurodevelopmental disorders are younger at diagnosis, 34 versus 38 years, p=0.004
- Seminoma patients with neurodevelopmental disorders present more often with more advanced stage disease, (more stage IV) Stage IV: 5.4% versus 1.2%, p=0.04**
- Znaor A, Skakkebaek NE, Rajpert-De Meyts E, Laversanne M, Kuliš T, Gurney J, et al. Testicular cancer incidence predictions in Europe 2010-2035: A rising burden despite population ageing. Int J Cancer. 2020;147(3):820-8.
- Gurney JK, Florio AA, Znaor A, Ferlay J, Laversanne M, Sarfati D, et al. International Trends in the Incidence of Testicular Cancer: Lessons from 35 Years and 41 Countries. Eur Urol. 2019;76(5):615-23.
- Rajpert-De Meyts E, McGlynn KA, Okamoto K, Jewett MA, Bokemeyer C. Testicular germ cell tumours. Lancet. 2016;387(10029):1762-74.
- Chen J, Sørensen HT, Miao M, Liang H, Ehrenstein V, Wang Z, et al. Cryptorchidism and increased risk of neurodevelopmental disorders. J Psychiatr Res. 2018;96:153-61.
- Butwicka A, Lichtenstein P, Landén M, Nordenvall AS, Nordenström A, Nordenskjöld A, et al. Hypospadias and increased risk for neurodevelopmental disorders. J Child Psychol Psychiatry. 2015;56(2):155-61.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in
This is an interesting observation.
The adverse prognosis in patients with psychiatric comorbidities is seen also in other malignancies, and calls for the need of extra support for these patient groups.