Leveraging AI and Neuroimaging to Uncover Early Signs of Alzheimer's Disease
Published in Neuroscience

One of the holy grails in dementia research is to catch people at the earliest possible stage, allowing for timely intervention with lifestyle changes or disease-modifying therapies. In reality this means picking up subtle changes well before symptoms are obvious. The difficulty of achieving such an early diagnosis has hindered clinical trials in dementia, including the commonest type of dementia, Alzheimer's disease [1, 2]. Recent evidence suggests that dementia pathology appears decades before symptoms appear [3, 4], raising the possibility of a window within which we can intervene to stop the disease before it causes serious damage.
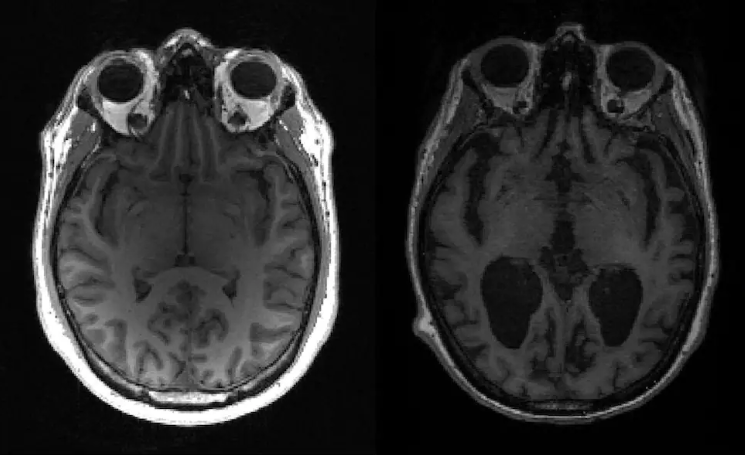
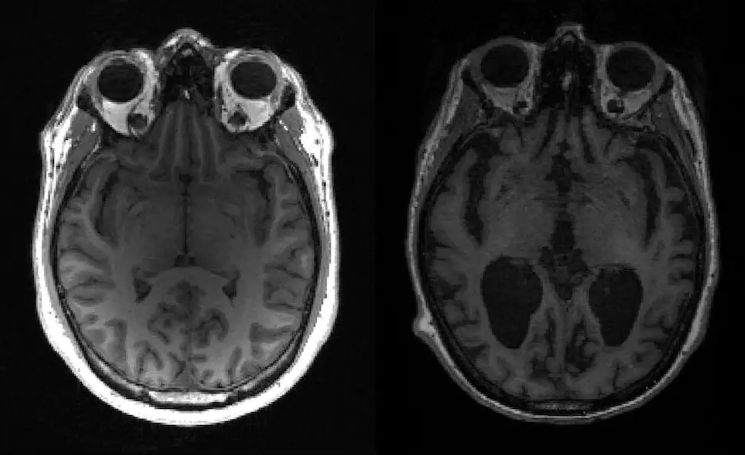
For a long time, MRI brain scans have been a key tool in diagnosing and understanding Alzheimer's disease. At the same time, we've also seen artificial intelligence (AI), particularly deep learning models, making a difference in various areas of medicine, including helping us answer many questions about the brain [5]. In our recently published work in Communications Medicine, we put forward an approach that harnesses AI and structural MRI brain scans to spot patterns of brain shrinkage that look like Alzheimer’s disease, but crucially in healthy individuals. This identifies a high-risk group that are likely to go on to Alzheimer's disease — exactly the group for recruitment to prevention studies and disease-modifying treatment trials.
Previous studies have picked up structural brain changes in rare genetic Alzheimer’s disease, but as far as we are aware this is the first study to do so in the common sporadic Alzheimer's disease.
Identifying High-Risk Individuals
AI approaches in structural MRI can identify Alzheimer's disease with a good degree of accuracy, but few such studies have validated their approach with a completely separate dataset [6, 7]. With this in mind, we used a carefully selected and well-characterised dataset of Alzheimer's disease to train our model (Alzheimer's Disease Neuroimaging Initiative dataset, ADNI), and a more “messy” clinical dataset with different diseases to check how well our model could handle the real-world situation (National Alzheimer's Coordinating Center, NACC).
Then, to identify a group of people at high risk of developing dementia, we use the validated model to find people with an MRI AI-derived pattern of Alzheimer's disease in a healthy cohort of over 37,000 people without a diagnosis of dementia from the UK Biobank study.
As shown in table 1, if you look at the negative predictive value, you can see that our model might miss some people with Alzheimer's but it's less likely to wrongly label healthy people as having the disease. Given that there is a lower rate of Alzheimer's in the UK Biobank data compared to ADNI and NACC, it's better to avoid wrongly classifying healthy people as having Alzheimer's. The performance of our model is best at the ADNI test set; this is expected given it is the cohort the model was trained on.

Implications for Early Intervention
Our AI-based analysis found people in the UK Biobank group who showed neuroimaging patterns similar to Alzheimer's, even though they didn't have a diagnosis or any reported symptoms of dementia. These people had an Alzheimer's-like pattern of brain shrinkage, indicating a high risk of developing the disease later on.
Being able to identify a high-risk group for Alzheimer's disease through AI and neuroimaging opens up new possibilities for early intervention and preventive measures. Researchers can design targeted prevention studies or early disease-modifying treatment trials for these people. Furthermore, our study found that individuals with the identified neuroimaging pattern had worse cognition in a pattern that looked like early Alzheimer’s disease. This reinforces the potential suitability of the identified cohort for screening and selection into clinical trials.
Importantly, the study also shed light on potentially modifiable risk factors associated with the neuroimaging phenotype. We found that people with Alzheimer-like scans identified by AI were more likely to smoke more, and had higher blood pressure. Smoking has long been recognized as a risk factor for dementia [8], and our study's results further support this association. Similarly, hypertension has been implicated in cognitive impairment, with midlife hypertension being a significant risk factor for developing dementia [9]. Both smoking and hypertension are eminently treatable.
The way forward
We believe that our approach of using AI with brain imaging and other measures provides a promising approach for identifying individuals at high risk of developing presymptomatic sporadic Alzheimer's disease. We have showcased the potential of AI algorithms to analyse complex neuroimaging data and detect subtle signs of Alzheimer's pathology before clinical symptoms arise. By leveraging AI's capabilities, we believe we have taken a significant step towards early detection and intervention in dementia research. In many ways our AI model is very simple - it is likely that by improving the model and adding more data, the accuracy can improve.
The identification of a high-risk cohort offers opportunities for preventive interventions and the design of tailored clinical trials. However, further research, validation, and longitudinal studies are necessary to fully understand the clinical implications and refine the performance of the AI model. With ongoing advancements in AI and neuroimaging technologies, we can remain hopeful that early intervention strategies will continue to evolve, bringing us closer to the goal of mitigating the devastating impact of Alzheimer's disease.
We hope our work inspires other researchers to try out these ideas with their own models and datasets. We've made our code publicly available to help with this.
References
[1] - Elmaleh, D. R. et al. Developing Effective Alzheimer’s Disease Therapies: Clinical Experience and Future Directions. Journal of Alzheimer’s Disease 71, 715–732 (2019).
[2] - Aisen, P. S., Vellas, B. & Hampel, H. Moving towards early clinical trials for amyloid-targeted therapy in Alzheimer’s disease. Nature Reviews Drug Discovery 12, 324–324 (2013).
[3] - Rohrer, J. D. et al. Presymptomatic cognitive and neuroanatomical changes in genetic frontotemporal dementia in the Genetic Frontotemporal dementia Initiative ( GENFI ) study : A cross-sectional analysis. Lancet neurology 14, 253–262 (2015).
[4] - Kinnunen, K. M. et al. Presymptomatic atrophy in autosomal dominant Alzheimer’s disease: A serial magnetic resonance imaging study. Alzheimer’s and Dementia 14, 43–53 (2018).
[5] - Yang, G. R. & Wang, X.-J. Artificial neural networks for neuroscientists: A primer. Neuron 107, 1048–1070 (2020).
[6] - Bzdok, D. & Yeo, B. T. Inference in the age of big data: Future perspectives on neuroscience 155, 549–564 (2017).
[7] - Bzdok, D., Varoquaux, G. & Steyerberg, E. W. Prediction, not association, paves the road to precision medicine 78, 127 (2021).
[8] - Peters, R. et al. Smoking, dementia and cognitive decline in the elderly, a systematic review. BMC Geriatrics 8, 36 (2008).
[9] - Rusanen, M., Kivipelto, M., Quesenberry, C. P., Jr, Zhou, J. & Whitmer, R. A. Heavy Smoking in Midlife and Long-term Risk of Alzheimer Disease and Vascular Dementia. Archives of Internal Medicine 171, 333–339 (2011).
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Public health and health governance in China
Publishing Model: Open Access
Deadline: Jul 31, 2026
Targeted diagnostics and therapies for autoimmune diseases
Publishing Model: Hybrid
Deadline: Oct 31, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in