Molecular stalking: liquid biopsies track down cancer in patients undergoing radiotherapy
Published in Cancer

In this work, published in British Journal of Cancer, we investigate the application of liquid biopsies, specifically the study of circulating tumour DNA (ctDNA), in cancer patients with low tumour burden treated by radiotherapy (RT). In the last decades, technology advances have fuelled a revolution in the accuracy of RT. However, in clinical routine, there are no molecular biomarkers to improve the personalization of these treatments. So, we hypothesized that the implementation of genomic profiling could redound on the stratification of RT patients to tailor treatments and surveillance protocols. To maximize our insights into this relatively unexplored niche of low tumour burden patients, in which good tissue biopsies can rarely be obtained, we applied a comprehensive approach that allowed us to assess the usefulness of liquid biopsy as alternative to tissue biopsies in Radiation Oncology decision-making.
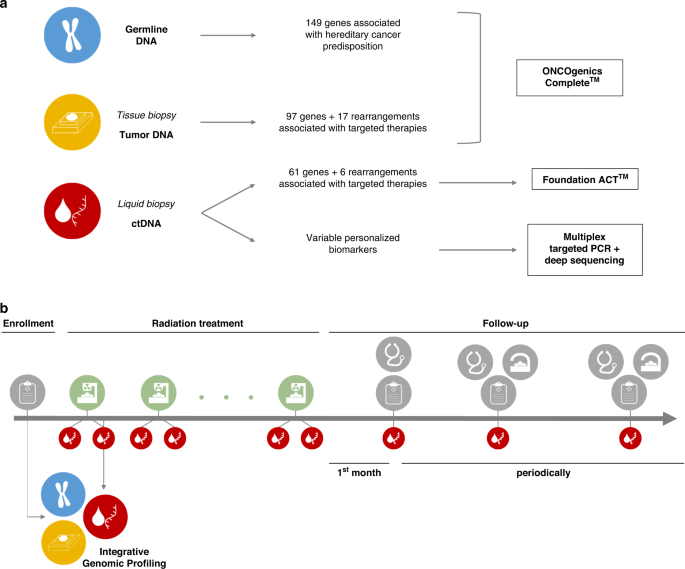
Genomic profiling can provide the physicians with not only information to select a specific drug, as most extended in clinical practice, but also molecular biomarkers to track the disease or predict risk/prognosis. We performed a comprehensive set of germline, tissue- and liquid-biopsy next generation sequencing (NGS) panels on 50 early-stage/oligometastatic cancer patients undergoing RT, and integrated the results to identify personalized genomic tumour biomarkers in each patient. Then, we used these biomarkers for longitudinal ctDNA monitoring in serial liquid biopsies collected during RT and follow-up.

Our results support the use of germline tests as a valuable complement for somatic studies, not only because of the potential detection of pathogenic germline variants that could be associated with hereditary predisposition to cancer (identified in 6.5% of patients of our cohort), but also because integration of the germline results allows to properly interpret the somatic results, especially those from liquid biopsy studies. This is particularly relevant in contexts of low tumour burden patients, with fewer variants and of lower allele frequencies. In our cohort, around one third of the variants identified by the liquid biopsy test were actually germline variants, whereas another third were variants derived from clonal haematopoiesis (somatic variants from haematological cells), living the remaining 1/3 as truly tumour derived. This information is essential for the correct selection of ctDNA biomarkers for follow-up. And a further advantage of using a fresh liquid biopsy before the selection of ctDNA biomarkers is that it allows to not only pick true tumour variants, but specifically those that are present in currently active lesions.
We also found that, in low tumour burden patients, somatic genomic studies on tissue biopsies and liquid biopsies are complementary but not completely concordant, which can be explained by spatial tumour heterogeneity, clonality or time elapsed between biopsies. The application of both tests in each patient would be the optimal scenario, but when tissue biopsies are not available, liquid biopsy is a good alternative to identify potential biomarkers or molecular targets of approved or under-development cancer therapies.
In total, more than one hundred genetic variants were selected as personalized ctDNA biomarkers. Our results show that longitudinal ctDNA analysis of well-curated somatic variants could be used as follow-up approach to track the disease in low tumour burden patients, even anticipating current gold-standard imaging diagnostic tests. Interestingly, the study of basal ctDNA levels (before the RT treatment) shows strong prognostic value, as it is associated to progression-free survival in our cohort, considering both early-stage and oligometastatic patients and regardless of the tumour lesion site. Basal ctDNA assessment stands as a promising biomarker to stratify the patients and help physicians in the decision to prescribe concomitant chemotherapy and/or intensify the RT treatment, which might lead to better patient management.
Precision Medicine, and particularly Precision Oncology as the standard bearer for the implementation of this trend in medicine, requires the integration of molecular and clinical information from different sources in an n-of-one context, where each patient is unique and multidisciplinary teams are needed. As far as we know, this is the first study addressing the real-time monitoring of ctDNA release throughout the entire RT treatment and follow-up, integrating a wide variety of clinical information and a comprehensive molecular testing approach. Further efforts are warranted to deepen into the clinical utility of liquid biopsies in different clinical contexts.
Our team, formed by molecular biologists, bioinformaticians, geneticists, radiation and medical oncologists and nurses, has joined forces and knowledge in this project to translate the research in liquid biopsies to the clinical routine. With the continued support of Fundación María Cristina Masaveu Peterson, we will try to keep on doing so to confirm and extend the relevant observations made in this work.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in