Please hack this nanodiagnostic
Published in Bioengineering & Biotechnology
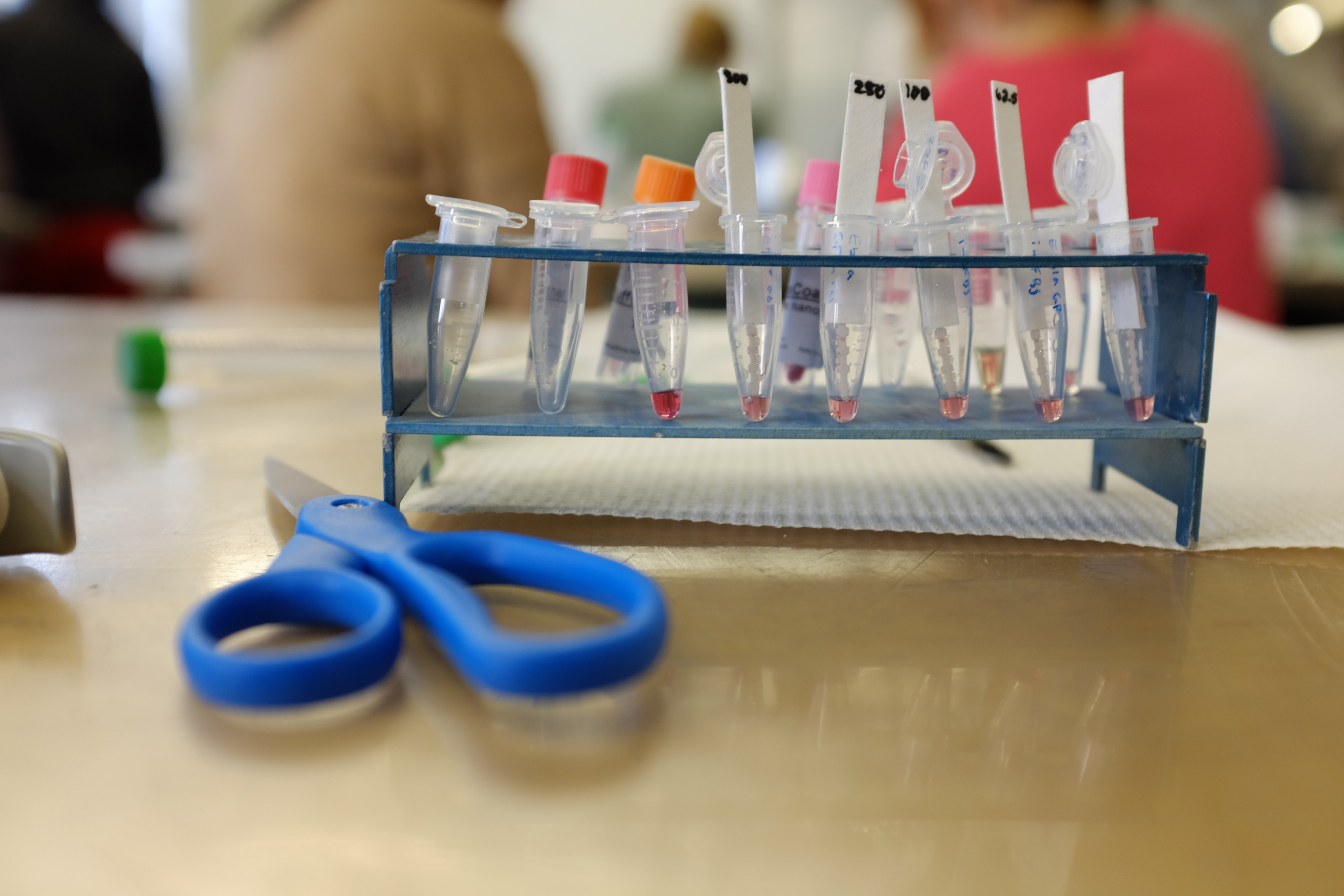

Last March, we started to get emails from some of the biggest hospitals in Boston—near our labs—to donate RNA extraction supplies, pipettes, and latex gloves to help them fight COVID-19. For us, the latex gloves were a signal that the extreme infectious disease disparities we’d seen in the places like Nicaragua and Ethiopia (where nurses often have to wash their one pair of gloves even in pre-COVID years), had arrived to the United States. In a globalized world, most of us have never experienced supply chain failures the way we saw them materialized in the Spring of 2020.
Diagnostics became one of the first areas to suffer, but it also became a tremendous source of learning across borders. Academic labs rushed to reconfigure their RT-PCR machines so that they could accept human samples, and pitched in their resources to shorten testing waiting times. This became a natural experiment in what happens when we shift diagnostics away from black box systems and into open hardware protocols.
Diagnostics are critical in the fight to infectious disease. They allow us to quarantine, inform treatment, and monitor the spread of a disease. Recent history shows that the lack of a diagnostic tool can spell disaster for millions of people. We’ve seen this movie before: Ebola, Zika, and Chagas outbreaks have all been subject to a mad scramble for diagnostic tools that arrived too late. We also know that these outbreaks are increasingly more frequent due to an increasingly connected world.
In our work in low-cost sensors, we have been using nanotechnology to improve on their ground diagnostic performance. Like other scientists in the field, we began with the notion of invention and shipping it, enhanced by user feedback from far away clinics in the developing world. Over time, a pattern emerged of epidemic -> proposals -> device -> epidemic -> proposals -> device, but missing was actual impact beyond the impact factor of a publication. The promise of nanotechnology for diagnostics is strong, but it’s far from meeting an equitable impact. So if informed design is not sufficient to create an impact for patients, how else can you democratize nanotechnology innovations so they aren’t just concentrated in wealthy countries? Epidemics do not know borders or check GDPs to enter a country. Everyone needs access to diagnostics, treatments, drugs and vaccines.
In our article (Gomez-Marquez and Hamad-Schifferli, 20211) we argue the need to rethink how diagnostics are made, and do away with the idea of self-contained black box systems. Black boxes can come in all sizes and price points: The multi-thousand dollar high throughput RT-PCR setup, to the $2 diagnostic test using gold nanoparticles. In both cases, there’s been a tradeoff between performance + price and local adaptability. Black box systems, even if they are easy to use, completely shut endusers from being able to make modifications. Nanotechnology-enabled diagnostic solutions can be unbundled into reconfigurable elements. This collective construction set can add agency to end users, where they tweak a final device, adapt it to the realities of their local supply chains and budgets, and increase the chance of local deployment.
How do we get nanotechnology solutions there? First, we let the enduser participate in the design process from the start. The traditional approach on this has been tons of user interviews so that a device can be informed by user feedback. Not every lab can ship a design team to remote towns in Nicaragua or Senegal. In contrast, we propose designing diagnostic test that are hackable. User feedback is replaced with user agency, so that local development can take place using reconfigurable elements in real time, and with repurposing of reagents such as antibodies and affinity agents, or synthesis of their own nanomaterials. We call this approach Design for Hack and we have used it over the last few years to push ourselves into generating adaptability and local development in the nanosensors we explore with users.

Who are these users? The stereotypical image of a remote village clinic or field hospital in a low to middle income country misses a much larger, and hopeful source of existing technical capacity: the diagnostic middleware workers. These are individuals staffing clinical labs throughout the developing world playing a critical role in disease diagnostics. In the absence of shiny automated machines, they functionalize protocols. They generate assays. And it is our belief and experience that they can also create nanotechnology-enabled diagnostics. Using desktop production techniques and open protocols, we can share techniques and knowledge to take advantage of a massively distributed manufacturing capacity, ready to learn and ready to treat.
1. Gomez-Marquez, J., Hamad-Schifferli, K. Local development of nanotechnology-based diagnostics. Nat. Nanotechnol. (2021). https://doi.org/10.1038/s41565-021-00907-2
Follow the Topic
-
Nature Nanotechnology
An interdisciplinary journal that publishes papers of the highest quality and significance in all areas of nanoscience and nanotechnology.


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in