CAR T-cell technology has revolutionized the management of refractory B-cell hematological malignancies. Since CAR T-cells targeting CD19 were first tested in patients with relapsed, refractory chronic lymphocytic leukemia and acute lymphoblastic leukemia, multiple studies have now demonstrated long-term remissions (e.g. potential cures) in all forms of B-cell malignancies1-3. Despite these exciting results, there are several limitations to CAR T-cell therapy including:
- Third-party manufacturing limits access to certified centers, and at the time of development of our trial (prior to commercial approval), CAR T-cell therapy was limited to only academic centers invited to participate in pharmaceutical sponsored trials or to those centers with large, expensive GMP facilities that could manufacture CARs internally.
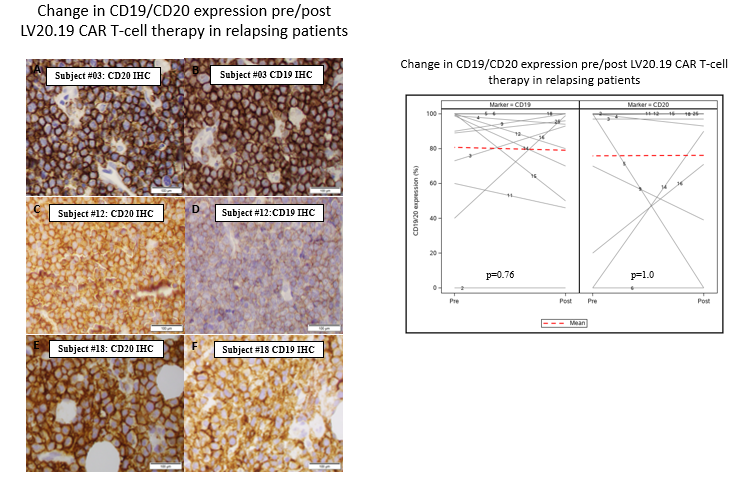
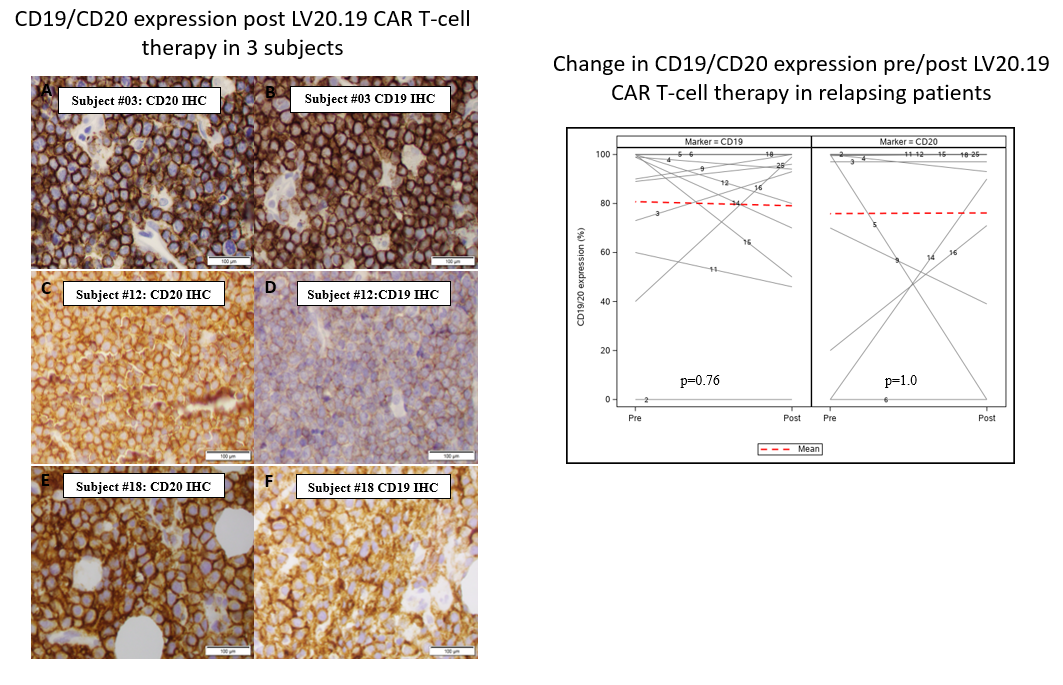
- Single targeting of the CD19 receptor was demonstrated to result in selective pressure against the antigen leading to clonal escape and development of a CD19 negative clone as a major cause of relapse4.
In this trial we attempted to overcome these limitations, by embracing new technology, specifically the CliniMACS Prodigy ® (Miltenyi Biotec) tabletop device, which allowed for production of CAR T-cells in a closed, GMP compliant environment within our cell therapy lab. This technology democratizes the manufacturing process allowing centers to collect, manufacture, and infuse CAR T-cells without third-party involvement. Further, in collaboration with Lentigen Technology we developed a Phase 1, first-in-human clinical trial testing a bispecific anti-CD19, anti-CD20 (LV20.19) CAR T-cell construct which by simultaneous dual antigen targeting aimed to limit CD19 antigen loss as a mechanism of resistance5.
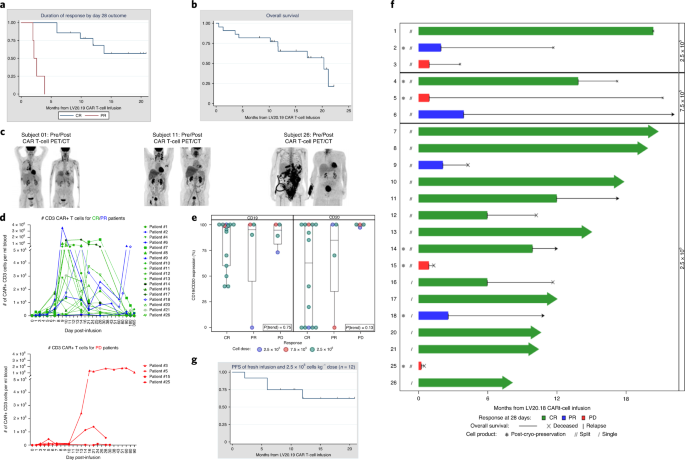
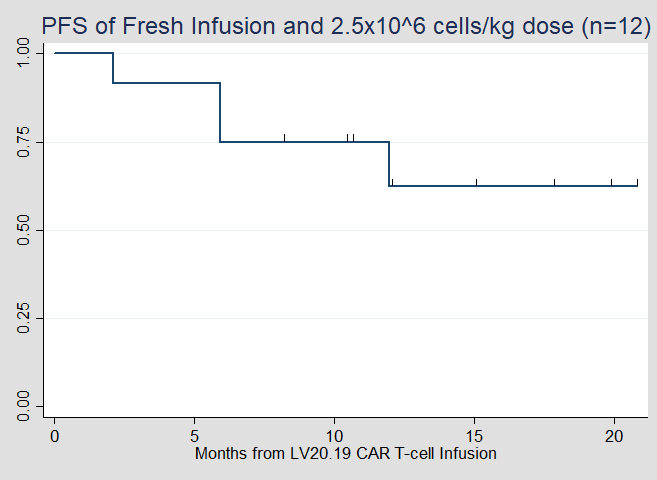
Prior to clinical enrollment on the study reported in this paper, we published our ability to use the Prodigy device to make functional CAR T-cells6. These data supported our IND application allowing us to launch our dose-escalation study of LV20.19 CAR T-cells. With little data on the safety of dual targeted CARs, our main prerogative was to limit toxicity. Accordingly, to reduce potential risks we started at a low cell dose of 2.5x105 cells/kg and split that infusion over 2 days in a 30%/70% fashion. To our surprise, the safety signal appeared to be as good or better than that reported for other CARs and we were able to quickly escalate to our target dose of 2.5x106 cells/kg with rapid transition to a single infusion. Through reliable in-house manufacturing, we initiated lymphodepletion during manufacturing with most of our patients receiving a fresh (non cryopreserved) infusion. We found that the subset of patients who received the target dose with fresh infusion had the best day 28 response rate (n=12, overall response 100%, complete remission 92%) with a median progression free survival that has not been reached.
Among patients who either did not respond or later relapsed post LV20.19 CAR T-cells, all were biopsied and interestingly they all retained CD19 expression, suggesting that bispecific CARs may limit antigen escape as a mechanism of relapse. We look forward to further testing these findings in a larger multi-center, Phase II clinical trial of non-cryopreserved LV20.19 CAR T-cells at a dose of 2.5x106 cells/kg in relapsed, refractory aggressive B-cell NHL. Our paper can be found at the following link: https://www.nature.com/articles/s41591-020-1081-3
- Wang M, Munoz J, Goy A, et al. KTE-X19 CAR T-Cell Therapy in Relapsed or Refractory Mantle-Cell Lymphoma. New England Journal of Medicine. 2020;382(14):1331-1342.
- Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. The New England journal of medicine. 2018;380(1):45-56.
- Maude SL, Laetsch TW, Buechner J, et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. New England Journal of Medicine. 2018;378(5):439-448.
- Shah NN, Fry TJ. Mechanisms of resistance to CAR T cell therapy. Nature reviews Clinical oncology. 2019;16(6):372-385.
- Schneider D, Xiong Y, Wu D, et al. A Tandem CD19/CD20 CAR Lentiviral Vector Drives On-Target and Off-Target Antigen Modulation in Leukemia Cell Lines. Journal for Immunotherapy of Cancer. 2017.
- Zhu F, Shah N, Xu H, et al. Closed-system manufacturing of CD19 and dual-targeted CD20/19 chimeric antigen receptor T cells using the CliniMACS Prodigy device at an academic medical center. Cytotherapy. 2018;20(3):394-406.
Follow the Topic
-
Nature Medicine
This journal encompasses original research ranging from new concepts in human biology and disease pathogenesis to new therapeutic modalities and drug development, to all phases of clinical work, as well as innovative technologies aimed at improving human health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Microbiome and energy metabolism
Publishing Model: Hybrid
Deadline: Dec 06, 2026
Digital Medicine for Infectious Diseases
Publishing Model: Hybrid
Deadline: Nov 09, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in