Soluble FRα: a potential biomarker for tumour expression, tumour burden and treatment response in ovarian cancer
Published in Cancer

Ovarian cancer
Ovarian cancer is the most lethal gynaecological malignancy, and survival rates remain poor. Currently, CA125 is the ‘gold standard’ serum biomarker for monitoring ovarian cancer. However, a key feature of ovarian tumours is intra‐tumour heterogeneity, meaning the co-existence within a single tumour of different cellular sub-clones, each sub-clone possibly harboring different cell markers. Therefore, using several complementary biomarkers to account for intra‐tumour heterogeneity, could improve surveillance and evaluation of response to treatment.
Folate receptor alpha (FRα)
FRα is a cell-surface glycoprotein expressed on a number of cancers, particularly ovarian cancer. Given that FRα can be shed from tumour cells and has been detected circulating in serum in soluble form (sFRα) we hypothesized that sFRα may have potential as an adjunct clinical biomarker for ovarian cancer.
FRα-targeted therapeutics
In addition to its potential role as a clinical biomarker, there has been significant interest in using FRa as a therapeutic target. Several therapies targeting FRα, such as the antibodies farleutuzumab and mirvetuximab soravtansine have been investigated in late-stage clinical trials, and our own FRα-targeting IgE therapeutic, MOv18 IgE, has recently been tested in a first-in-class, Phase 1 clinical trial. Despite promising results, no FRα-targeted agents are yet approved for patients with ovarian cancer. This may be due to challenges in selecting patients likely to respond to treatment. Although immunohistochemical (IHC) staining of tumour samples is commonly used to determine FRα protein expression, we asked whether a sFRα-based assessment of FRα tumour expression might be complementary. We therefore sought to evaluate the potential correlations between sFRα and the degree of tumour FRα expression, and to consider whether sFRα levels are influenced by cancer treatments.
What we investigated
We used IHC to determine tumour FRα expression status (N=316 ovarian tumours) and ELISA to measure FRα in serum samples (N=143) taken longitudinally from patients, before and during neo-adjuvant, adjuvant and palliative chemotherapy. We investigated the relationship between sFRα and tumour FRα, as well as with tumour burden (defined using a bespoke scoring system, with the aim of capturing the volume of disease in its entirety). Lastly, we evaluated the potential impact of free circulating FRα on efficacy of the FRα-specific IgE therapeutic, MOv18 IgE, using an antibody-dependent cellular cytotoxicity (ADCC) assay.
 Figure 1: Study design and sample workflow.
Figure 1: Study design and sample workflow.
Key Findings
Within our diverse ovarian cancer patient cohort, 53% of tumours were positive for either membrane or cytoplasmic FRα staining, or both, with this percentage rising to 60% in high-grade serous ovarian cancers. Levels of sFRα were significantly greater in sera of patients (5.7 ± 0.9 ng/ml) compared with sera from healthy controls (1.4 ± 0.6 ng/ml), and significantly higher in sera from patients with FRα-positive tumours (7.6 ± 1.8 ng/ml), compared to those with FRα-negative tumours (2.6 ± 1.2 ng/ml). Furthermore, the baseline level of circulating sFRα in treatment-naïve patients was predictive of positive tumour cell membrane FRα expression (receiver operating characteristic (ROC) curve analysis: AUC=0.76, P=0.007).
In those patients with detectable levels of circulating sFRα at the start of treatment, sFRα levels significantly decreased over the course of neo-adjuvant and palliative treatment, in line with a reduction in disease burden. ROC curve analysis showed that levels of sFRα in sera from treatment-naïve patients were associated with high tumour burden (AUC=0.74, P=0.005).
Overall, these findings suggest that longitudinal sFRα levels may be reflective of the patients’ disease burden, and changes in disease burden following standard therapies.
Finally, we looked at whether the efficacy of anti-FRα treatments may be inhibited by the presence of free FRα in the circulation.The ADCC of FRα-expressing cancer cells by human immune cells mediated by low concentrations of MOv18 IgE was significantly reduced by high concentrations of free, recombinant FRα. However, ADCC mediated by MOv18 IgE at cancer cell-saturating concentrations was not perturbed by the presence of even the highest levels of FRα.
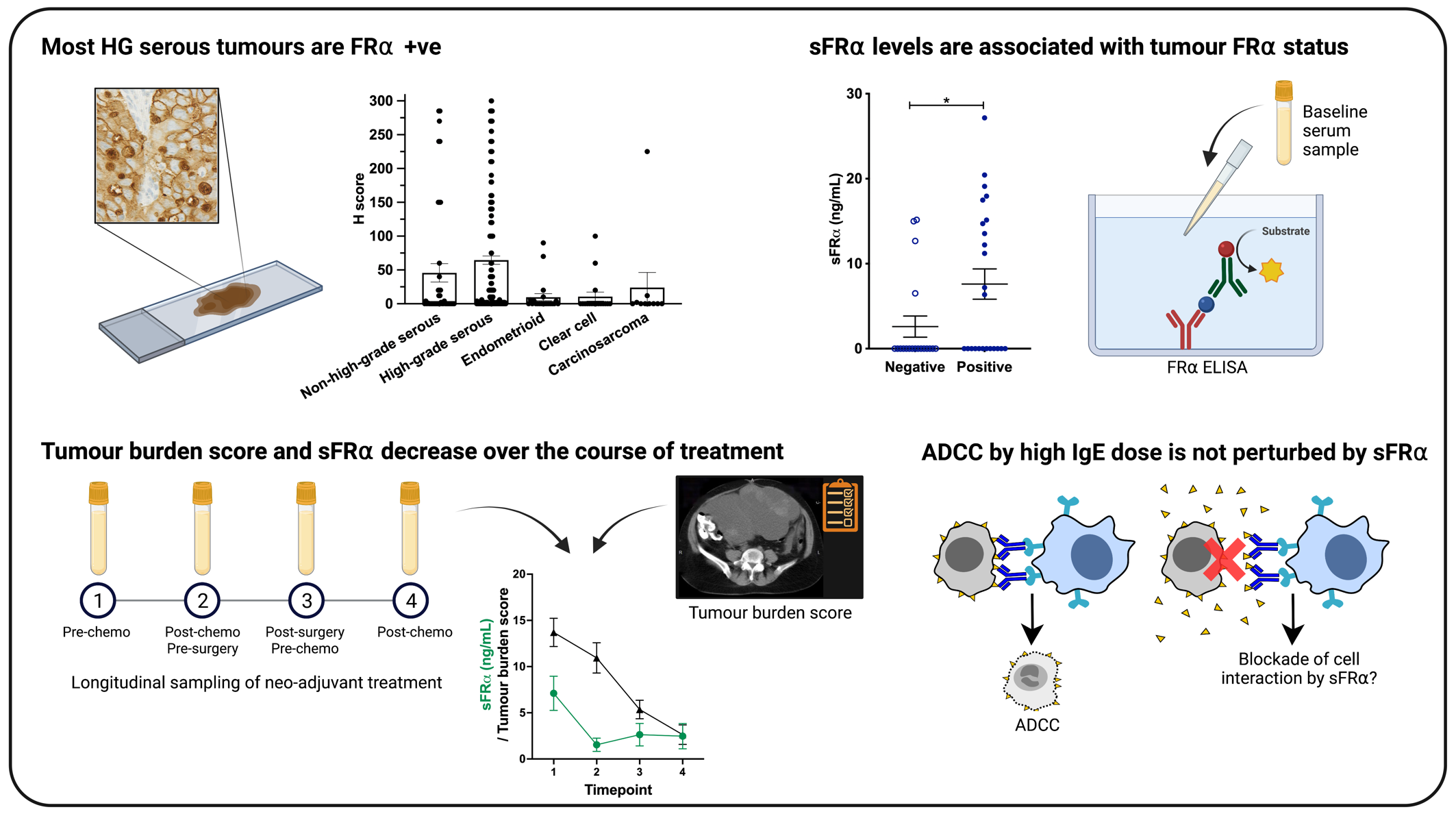 Figure 2: Graphical summary of key findings.
Figure 2: Graphical summary of key findings.
Conclusions and Translational Impact
Our data suggest that sFRα may present a useful and dynamic non-invasive marker for tumour FRα expression. Furthermore, sFRα could be used to evaluate disease burden and monitor response to treatment in some patients, as well as help in the selection of patients to receive potential FRα-targeting therapies.
Since our analyses were performed on a limited number of patient samples, future studies in larger datasets are required.
Importantly, our data also showed that at higher antibody concentrations, the anti-tumoural potency of the anti-FRα antibody, MOv18 IgE, was unaltered by even the highest levels of sFRα, suggesting that the number of antigen-binding sites on the antibody outweighed any blocking effects of free FRα antigen and were thus sufficient to trigger cancer cell cytotoxicity. Therefore, to overcome any decoy functions of sFRα on future clinical applications of anti-FRα therapies, it may be necessary to increase the required therapeutic dose in the minority of patients with the greatest levels of sFRα.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in