Afatinib as Neoadjuvant Treatment for Stage III EGFR-Mutant Non-Small Cell Lung Cancer (TEAM-LungMate 004): A Prospective, Single-Arm, Phase II Study
Published in Cancer
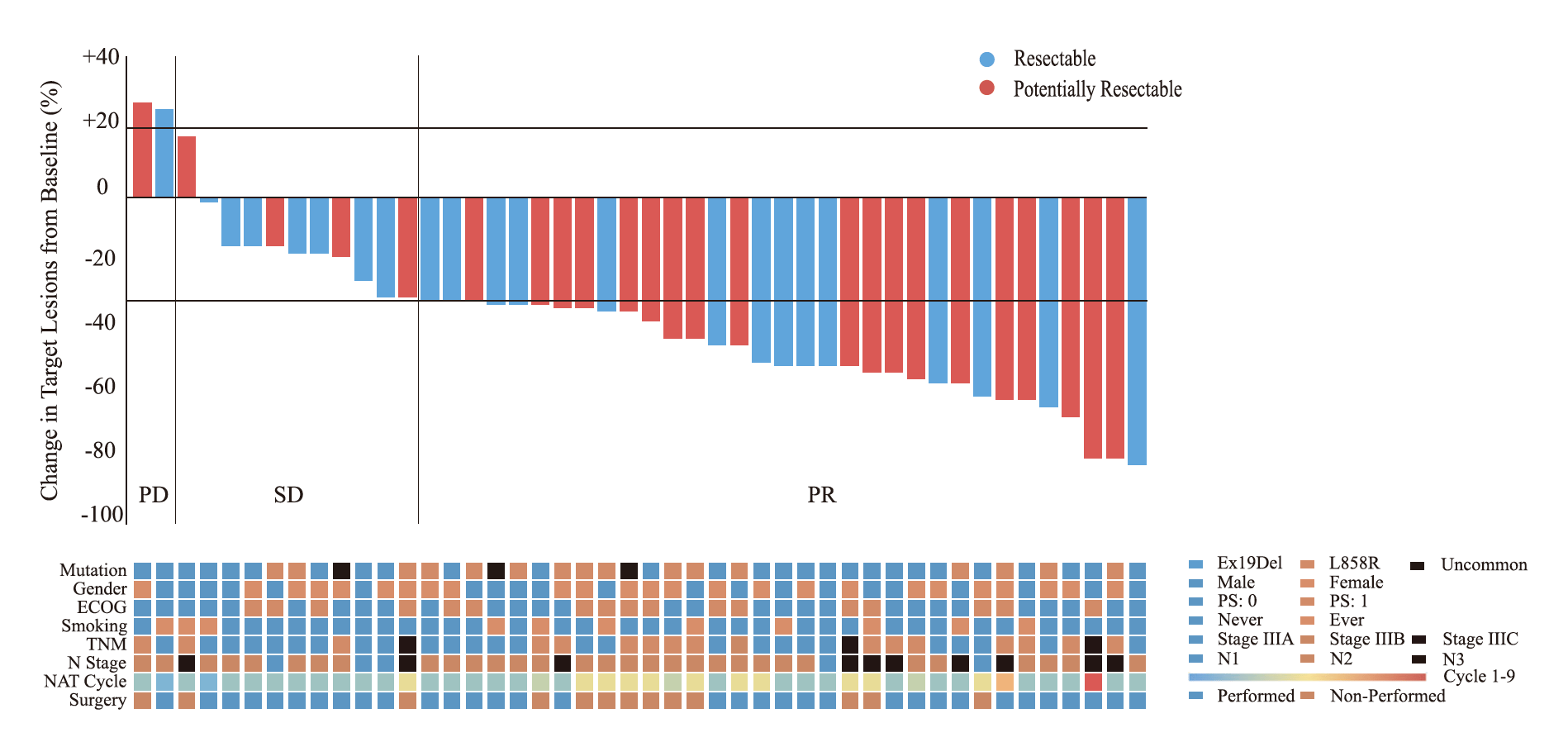

The ORR, was 70.2% (95% CI: 56.5%-84.0%) met the pre-specified primary endpoint. There were 33 patients received surgery after neoadjuvant treatment. The MPR, pCR, pathological downstaging, and R0 rates were 9.1%, 3.0%, 57.6%, and 87.9%, respectively.
Safety
All participants (100%) experienced TRAEs, but no grade 5 TRAEs were observed. Grade 3/4 TRAEs occurred in 3 patients (6.4%), including diarrhea, interstitial pneumonia, and hepatic impairment, respectively. Discontinuation of Afatinib was observed in only one patient due to grade 4 diarrhea. The most common TRAEs during NAT were diarrhea (78.7%), rash (78.7%). Surgery-related complications occurred in 4 patients, including prolonged air leakage (9.1%) and bronchopleural fistula (3.0%). No surgery-related death occurred within 90 days postoperatively.
Efficacy Associated Molecular Characteristics for Afatinib
By IHC score, the expression of programmed cell death 1 ligand 1 (PD-L1) in primary tumor after NAT was significantly higher than those in baseline (p = 0.013), and this trend was validated in the evaluation of 5 paired samples before and after Afatinib treatment. By RNA-seq, “T cell receptor signaling” pathway was significantly enriched in responsive tumor samples, indicating T-cell activation and CD8+ T-cells infiltration after Afatinib treatment in responsive patients. Additionally, an increasing tendency of B-cells was observed after Afatinib treatment drainage lymph node samples in responsive patients. Finally, the changes in the tumor microenvironment (TME) between different response groups after Afatinib treatment were observed. Several immune cells including T-cells, cytotoxic lymphocytes, B-cells, and NK cells were higher in responders.
Afatinib as a single-agent neoadjuvant therapy for stage III EGFR-mutant NSCLC offers a favorable objective tumor response and has an acceptable toxicity profile in clinical practice. Dynamic changes in TME are observed, particularly in responders, which may have implications for identifying predictive markers for EGFR-TKI treatment and guiding the future clinical trials.
1. Goldstraw P, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 11, 39-51 (2016).
2. Zhao Y, et al. Efficacy and safety of first line treatments for patients with advanced epidermal growth factor receptor mutated, non-small cell lung cancer: systematic review and network meta-analysis. BMJ 367, l5460 (2019).
3. Mitsudomi T, Suda K, Yatabe Y. Surgery for NSCLC in the era of personalized medicine. Nat Rev Clin Oncol 10, 235-244 (2013).
4. Greenhalgh J, et al. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. The Cochrane database of systematic reviews 3, CD010383 (2021).
5. Li S, et al. Cytokine-induced Src homology 2 protein (CIS) promotes T cell receptor-mediated proliferation and prolongs survival of activated T cells. J Exp Med 191, 985-994 (2000).
6. Boudin L, et al. CISH Expression Is Associated with Metastasis-Free Interval in Triple-Negative Breast Cancer and Refines the Prognostic Value of PDL1 Expression. Cancers (Basel) 14, (2022).
7. Miah M, Yoon C, Kim J, Jang J, Seong Y, Bae Y. CISH is induced during DC development and regulates DC-mediated CTL activation. European journal of immunology 42, 58-68 (2012).
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Jun 01, 2026
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in