Current state of ethical challenges reported in Saudi Arabia: a systematic review & bibliometric analysis from 2010 to 2021
Published in Healthcare & Nursing and Philosophy & Religion

Bioethics comprises principles that focus on medical/ clinical ethics (issues in healthcare), research ethics (issues in conduction and implications of research), environmental ethics (issues that arise due to relationships between human activities and the environment), and public health ethics (issues in public health). Moral action guides and principles are important in providing guidance to the moral duties in any situation. Although not absolute, such guidelines need to be acceptable among different religions and cultures.
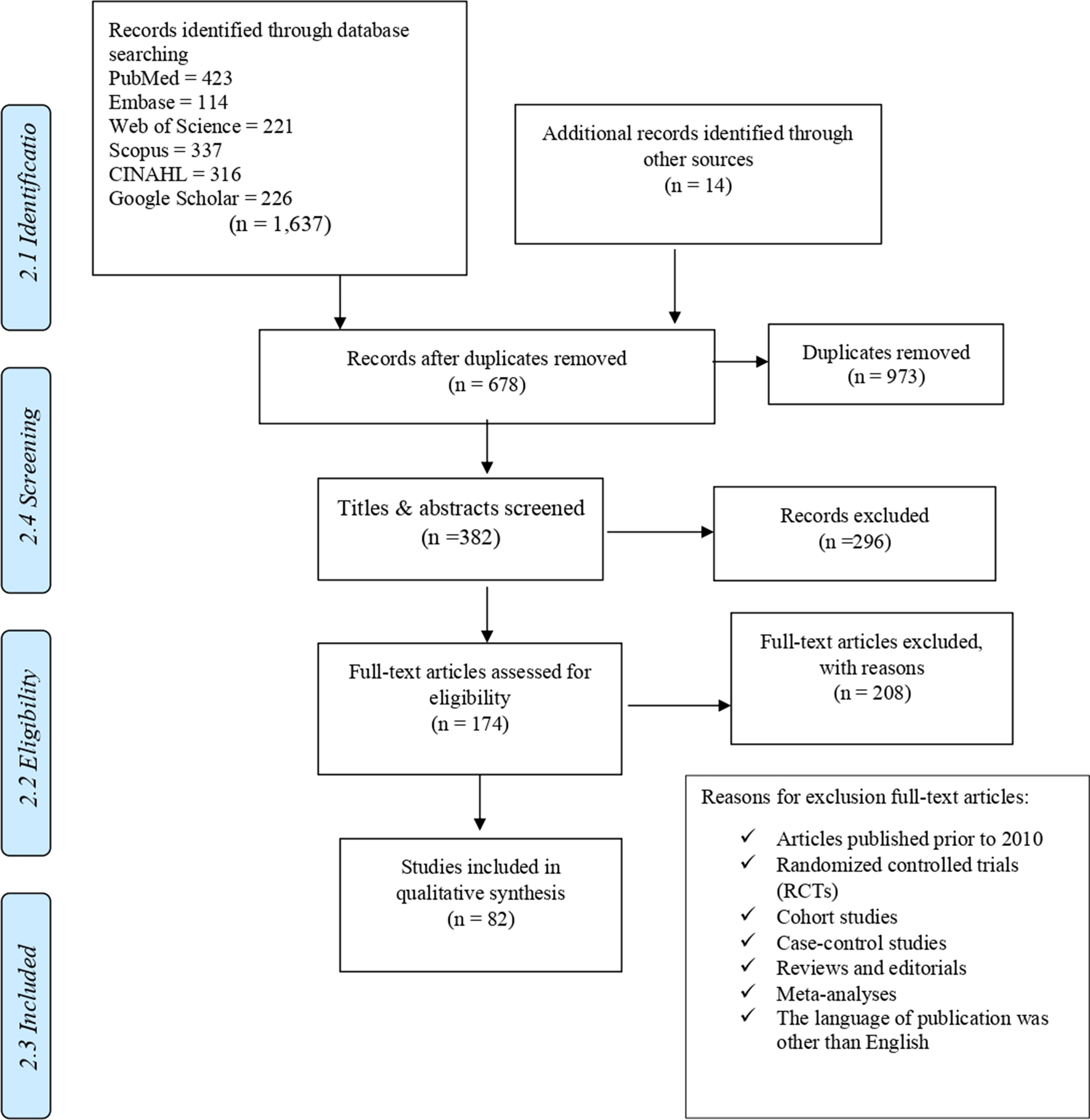
In Saudi Arabia, bioethical issues often challenge ethics, as they contradict moral traditions and sometimes perceive matters in an unconventional light, which must take the entire spectrum of ethical theories into account. For this reason, consideration of the moral and philosophical aspects of bioethics is of great importance. Therefore, this systematic review aimed to systematically identify, compile, describe and discuss ethical arguments and concepts in the best-studied domains of bioethics in Saudi Arabia and present cultural, social, educational, and humane perspectives. As a result, this systematic review became the first organized synthesis of the five most debated bioethical domains that have been studied in the Kingdom of Saudi Arabia. Eighty-two studies were identified across five main domains for a final review and assessment: 'Medical Ethics Curriculum in Saudi Arabia,' 'Doctor-Patient Relations,' 'Informed Consent,' 'Do-Not-Resuscitate,' 'Organ Donation & Transplantation.'
The most studied domain of five included domains was ‘Organ Donation and Transplantation,’ 33 articles, with the most papers being published in 2020. The overall knowledge about organ donation and transplantation varied based on the research objective (i.e., blood, skin, kidney donation). In general, the participants reported insufficient information about organ donation and transplantation. The main source of information about organ donation was TV, social media. Participants from rural areas were less likely to have information about organ donation than their counterparts in urban areas. Organ donation awareness was higher in educated individuals with higher socioeconomic status and married participants. The degree of awareness was found to impact the willingness to donate positively. Reasons for refusal to donate were the fear of premature termination of medical treatment to facilitate organ retrieval and transplantation, worries about receiving inadequate health care after donation, lack of family support, lack of incentives, not enough information about organ donation, fear of complications after organ donation, religion. In contrast to the stated barriers to organ donation, among those participants who expressed their will or were positive about organ donation and transplantation, gender, age of the recipient, religion and incentives did not appear to play a role. Moreover, organ donation was motivated by helping others and compassion, a good deed, the importance of donation, belief that organs are not beneficial after death, and an altruistic act.
The synthesis of ‘Medical Ethics Curriculum in Saudi Arabia’ domain showed that regardless of the region, target population, most participants in all included studies agreed on the importance of studying the principles of medical ethics as a discipline with its methods, literature, vocabulary, and content. Although some participants completed theoretical ethics classes while attending medical school, the theory does not address the practical ethical dilemma faced in daily practice after graduation. There was a lack of knowledge about organ donation regulations, withholding or stopping mechanical ventilation, conflict with family, and advice from the ethics committee, religious aspects, brain death, 'Do-Not-Resuscitate (DNR) policies, the existence of the Saudi PBR.
The thematic evaluation of 'Doctor-Patient Relations' domain showed that most participants, mainly healthcare representatives had little knowledge about doctor-patient relations. However, there was a strong consensus that every patient should be treated with honesty and dignity. Patients of a high socioeconomic class should not be treated with extra care, and confidentiality should be maintained in all circumstances. Lack of training, knowledge of cultural norms, patient participation in decision-making, gender differences between patients and doctors, and a lack of time were major barriers to effective communication skills with patients and their families. Patients recommended doctors and nurses to improve their interpersonal skills and take a more holistic, patient-centered approach. This can improve information delivery and resolve disagreements between patients/family members and healthcare providers about treatment decisions.
The third most studied domain of medical ethics research in Saudi Arabia was 'Informed Consent' with 12 publications. Health care providers supported informed consent. The majority agreed that consent should be given for each new procedure and should be perceived as an ongoing process, not a one-off decision, with parental consent being considered mandatory for children's treatment. However, there was low quality of informed consent in terms of experience with informed consent processes and transparency of risks. Although patients' opinions on the purpose of informed consent varied, the informed consent process and being aware of treatment was important for all. In terms of the trust, some patients trusted the doctor to make decisions on their behalf, while others required more independent decision-making and preferably more effective disclosure of information. In addition, there was an overall poor quality of informed consent process and administration, knowledge of the risks of intervention and alternative treatment, and insufficient information included in informed consent.
The synthesis of ‘Do-Not-Resuscitate’ domain showed that most healthcare representatives could define the order of DNR. Still, it required deeper knowledge to learn whether there is a clear local or national DNR policy. Those who knew about the policy did not read in detail. The most common limitation of essential discussions about DNR was a lack of patient understanding, educational level, cultural background of patients, and a lack of DNR policy knowledge by medical staff. Most health care representatives wanted to learn more about patients' rights regarding end-of-life care and the use of the DNR order, as this would support the treatment plan for terminally ill patients. Studies in which patients were included as a target population expressed a will to participate in discussions with doctors on planning end-of-life care and making their own decisions. Patients with higher levels of education, medical background, and knowledge of DNR were more likely to agree with DNR practice. Non-Saudi doctors making decisions about life-sustaining treatment or DNR orders consulted with ethics committees in their hospitals more often than Saudi doctors. Saudi doctors who received their education and postgraduate studies abroad were confident in their knowledge of ethics in medical practice but were less confident in making decisions about life-sustaining treatment or DNR orders.
This systematic quantitative synthesis is expected to guide researchers, funders, and policymakers about the strengths and gaps in knowledge and attitudes regarding medical ethics in Saudi Arabia, both among the general public and health professionals.
Follow the Topic
-
BMC Medical Ethics

This journal is an open access journal publishing original peer-reviewed research articles in relation to the ethical aspects of biomedical research and clinical practice, including professional choices and conduct, medical technologies, healthcare systems and health policies.
Related Collections
With Collections, you can get published faster and increase your visibility.
Moral status and ethical implications of abortion
The moral status and ethical implications surrounding abortion have been subjects of intense debate across various cultural, religious, and philosophical contexts. Addressing the ethical dimensions of abortion is essential for developing frameworks that support informed decision-making and respect for diverse beliefs. Recent advancements in bioethics have fostered a more nuanced understanding of reproductive choice, leading to improved policies and practices that prioritize women's health and autonomy. Additionally, the societal impact of landmark legal cases, such as Roe v. Wade, continues to shape the discourse on reproductive rights, emphasizing the importance of ongoing examination of ethical principles in this arena.
BMC Medical Ethics is calling for submissions to our Collection on Moral status and ethical implications of abortion. This Collection seeks to explore the complexities of abortion ethics, including questions of maternal autonomy, reproductive justice, and the competing moral frameworks that inform individuals’ and societies’ views on this critical issue. Key topics of interest for submission include, but are not limited to:
Maternal autonomy in reproductive decision-making
Reproductive justice and abortion rights
Moral conflict and abortion ethics
Religious perspectives on abortion
Societal impact of Roe v. Wade
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Apr 02, 2026
Global health equity and ethics
BMC Medical Ethics invites submissions to our new Collection, Global health equity and ethics. The concept of global health equity encompasses the moral principles that guide health policies and practices aimed at reducing disparities in healthcare access and outcomes among different populations. As the world becomes increasingly interconnected, ethical considerations surrounding health equity are more critical than ever.
Promoting health equity is an ethical imperative in public health. As social determinants continue to drive disparities, public health ethics and ethical advocacy are essential to ensuring that policies and interventions are not only effective but also just. We encourage research that confronts these ethical challenges and supports a more equitable healthcare landscape.
This Collection welcomes submissions that explore the ethical dimensions of health equity, examining the systemic barriers that marginalized populations face and how these barriers can be dismantled to promote equitable healthcare for all. Key topics of interest for submission include, but are not limited to:
Ethical considerations in healthcare access
Addressing global disparities in health outcomes
Health justice and marginalized populations
Social determinants of health and health inequities
Policy implications for equitable healthcare
This Collection supports and amplifies research related to SDG 3: Good Health and Well-Being, SDG 10: Reduced Inequalities, and SDG 16: Peace, Justice and Strong Institutions.
All manuscripts submitted to this journal, including those submitted to collections and special issues, are assessed in line with our editorial policies and the journal’s peer review process. Reviewers and editors are required to declare competing interests and can be excluded from the peer review process if a competing interest exists.
Publishing Model: Open Access
Deadline: Jun 30, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in