European Public Health Week 2026: Why defining advocacy matters (and why we almost took it for granted)
Published in Public Health, Behavioural Sciences & Psychology, and Arts & Humanities
In health and public health, advocacy is one of those words that feels immediately familiar.
It appears everywhere: in conversations about health equity, patient engagement, professional responsibility, policy change, and community action. It is present in institutional strategies, training frameworks, and everyday professional language. It is widely treated as something essential, almost self-evident.
And yet, as European Public Health Week 2026 invites us to reflect on how health systems can become more equitable, participatory, and responsive, a fundamental question becomes harder to ignore: do we really share a clear understanding of what advocacy means?
When we began working on this paper, we thought we did. But the more we explored the literature, the less certain we became.
That realization was not immediate. At first, advocacy seemed like a stable concept - widely used, broadly understood. But as we started examining the literature more systematically, a different picture emerged. Advocacy was not only central to many discussions in healthcare and public health; it was also surprisingly underdefined.
This tension - between importance and ambiguity - became the starting point of our study.
A simple question that turned out to be complex
We began with what seemed like a straightforward question:
What do we actually mean when we talk about advocacy in public health and healthcare?
This was not just a conceptual curiosity. It had very practical implications. Across many contexts, advocacy is increasingly expected - from health professionals, patient representatives, community leaders, and civil society actors. It is often described as a core competence, a professional duty, or even an ethical imperative.
But if something is expected, it should also be clear enough to be supported, taught, and evaluated.
Otherwise, it risks remaining a powerful but vague idea - something we all agree is important, but struggle to translate into practice.
Looking across disciplines and practices
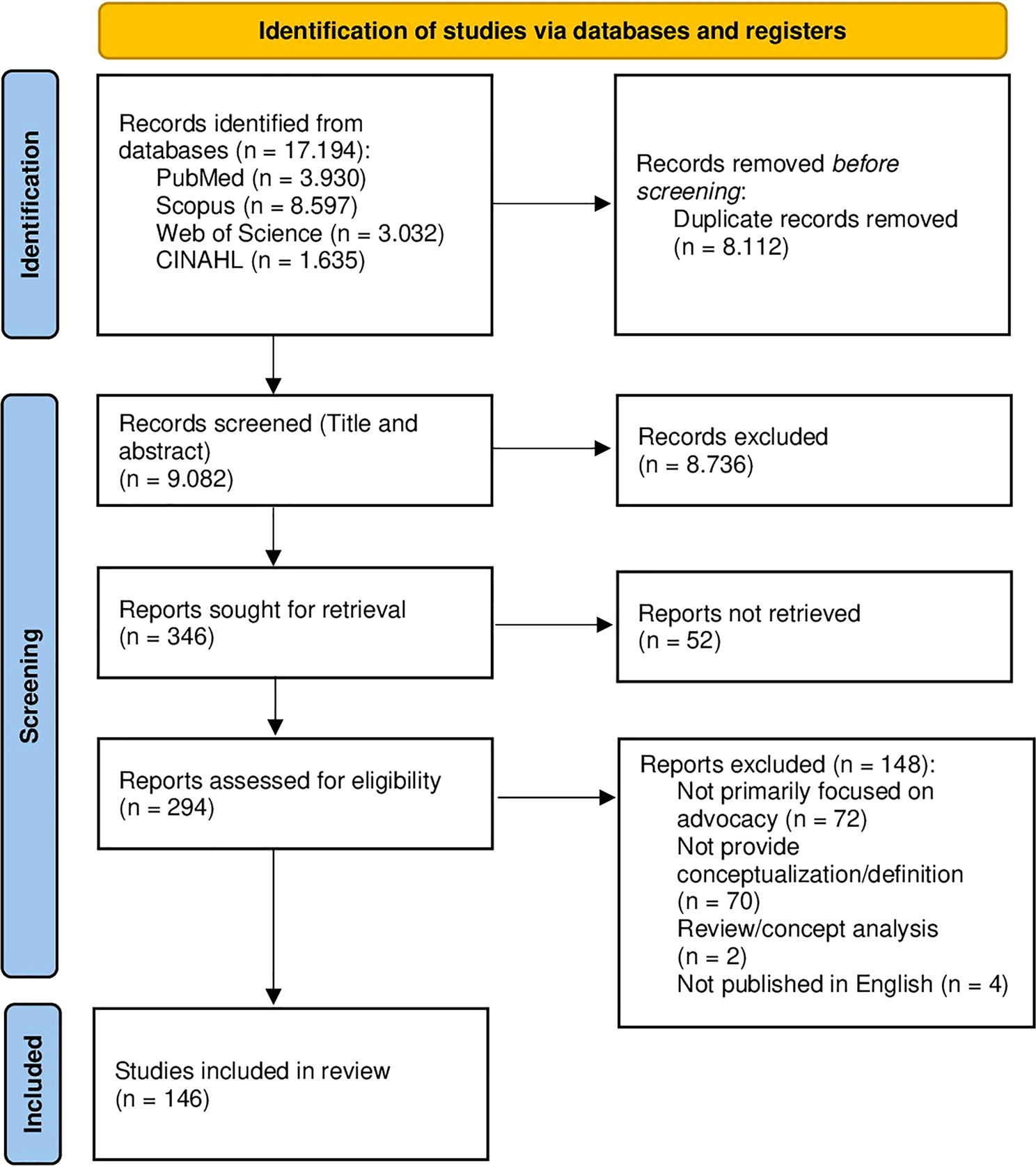
To explore this issue, we conducted a scoping review across multiple domains, including healthcare, public health, education, and social and policy research.
Rather than focusing on a single profession or type of action, we deliberately took a broad perspective. Advocacy is not confined to one role or setting, and we wanted to reflect that diversity. In total, we included 146 documents.
What we found was both reassuring and challenging.
A shared vision - at least in principle
On one level, the literature was remarkably consistent.
Across different contexts, advocacy was closely associated with values such as equity, social justice, participation, and systemic change. It was rarely described as simply helping individuals navigate services. More often, it was framed as something broader: a way to address structural barriers, amplify marginalized voices, influence institutions, and connect lived experiences with decision-making processes.
In that sense, there was a strong shared vision. Advocacy was presented as a necessary component of more inclusive and responsive health systems.
But many meanings, many roles, many practices
At the same time, however, this coherence did not extend to definitions or operational models.
Advocacy could mean many different things: supporting individual patients, mobilizing communities, engaging in policy processes, initiating legal action, working with the media, or contributing to education and awareness.
It could be carried out by healthcare professionals, patient groups, community actors, or organizations. It could take place at the bedside, in local communities, or at national and international policy levels.
This diversity is not a problem in itself. On the contrary, it reflects the richness and adaptability of advocacy.
But it also creates a challenge.
When a single term is used to describe such a wide range of activities, without sufficient conceptual clarity, it becomes difficult to build shared expectations. What does advocacy actually require? What are its boundaries? What should it achieve?
These questions are not always explicitly addressed.
The missing piece: how do we evaluate advocacy?
This lack of clarity became even more evident when we looked at evaluation.
Although advocacy is widely recognized as important, very few studies reported concrete ways to assess it. Only a small minority of the papers we included referred to specific measurement tools - and none of these was standardized.
In many cases, advocacy seemed to function as a normative concept: something that should matter, rather than something that is systematically examined.
For us, this was one of the most striking findings.
It suggests that while advocacy has gained visibility and legitimacy, the methodological tools needed to support it have not developed at the same pace.
Growing expectations, uneven foundations
This gap becomes particularly relevant in the current context.
Health systems are increasingly called to be more participatory, more inclusive, and more responsive. There is growing emphasis on patient involvement, community engagement, and equity-oriented approaches.
Advocacy is often positioned at the heart of these transformations.
And yet, the infrastructures that would allow advocacy to be practiced, supported, and evaluated in a consistent way remain uneven. Expectations are rising, but the conceptual and methodological foundations are still fragmented.
From mapping to proposing a way forward
Our goal, therefore, was not only to map how advocacy is described in the literature, but also to contribute to a more structured conversation about its future.
Based on our findings, we developed a preliminary framework for equity-oriented public health advocacy. This framework brings together several interconnected dimensions:
- a clear normative grounding in values such as equity and justice
- a multilevel perspective that connects individual, community, and systemic action
- attention to relational and communicative practices
- the development of critical and systemic literacy
- a form of professionalism that includes reflexivity and civic agency
- and, importantly, mechanisms for evaluation and accountability
We do not present this as a definitive model. Rather, it is a starting point—a way to make the concept of advocacy more explicit, more discussable, and more operational.
Beyond “speaking up”
One of the risks we identified is reducing advocacy to a generic idea of “speaking up.”
While voice is certainly important, advocacy is more complex than that.
It involves navigating relationships, understanding systems, interpreting contexts, and connecting individual or collective experiences with broader institutional change. It requires not only motivation, but also knowledge, skills, and supportive environments.
If these dimensions remain implicit, advocacy may continue to be celebrated in principle while under-supported in practice.
A shared space between professions and society
Another important insight from our review is that advocacy does not belong to a single group.
It is not only the responsibility of individual professionals, nor is it confined to formal institutions. It exists at the intersection of professional roles, civic action, and public accountability.
This is precisely why defining it more clearly matters.
Clarification is not about limiting advocacy, but about making it more visible, more teachable, and more sustainable.
A final reflection
As a scoping review, our study does not resolve all the ambiguities surrounding advocacy. Nor should it. Different contexts will always call for different forms of action.
But if there is one message we hope readers will take away, it is this:
Advocacy has become too important to remain conceptually vague.
Defining it more carefully is not just an academic exercise. It is part of building health systems that are more equitable, more accountable, and more connected to the realities of the people they serve.
And perhaps, in the end, that is what advocacy is really about.
Follow the Topic
-
International Journal for Equity in Health
This journal presents evidence relevant to the search for, and attainment of, equity in health across and within countries and publishes research which improves the understanding of issues that influence the distribution of health and healthcare within populations.

Related Collections
With Collections, you can get published faster and increase your visibility.
Racism and Health
The ongoing advancement of our understanding of how racism impacts health - both directly and structurally - is crucial for addressing the deep-rooted health inequities that persist globally. Structural racism shapes health outcomes among racialized populations, contributing to inequities in healthcare access and quality, and impacting social, political, or environmental determinants of health. Existing research also connects direct and visible manifestations of racism, such as major and everyday discrimination, to negative health outcomes. At the same time, racism does not operate in isolation. A growing body of research shows how it intersects with other systems of oppression—such as classism and patriarchy—and with broader social determinants of health, producing compounded and context-specific inequities. An intersectional lens is therefore essential to understand how overlapping structures of power and exclusion shape health and healthcare experiences. These insights are essential in conducting rigorous and thorough health research, guiding anti-racist health policy, and ultimately, ensuring equitable health for all.
Looking forward, research holds the potential to develop new methodologies and indices and unveil complexities in how racism manifests within healthcare systems and societal structures. By deepening our collective understanding, we can develop more effective interventions that target the root causes of health inequities.
We invite researchers to contribute to this special Collection on Racism and Health, focusing on advancing our understanding and addressing health inequities. Topics of interest include but are not limited to:
- Racism as a structural determinant of health
- Racism as a direct determinant of health
- Racialized health outcomes in different populations
- Intersectionality and inequities in health, healthcare access and quality
- Nexuses between social, political, and environmental determinants of health and systemic discrimination
- Anti-racist health policy frameworks and systems
- Impact of racism on mental health
- Health inequities in reproductive, maternal, and child health
- Obstetric and reproductive violence
- Community-based interventions for equitable health
- Decolonizing health research and global health epistemologies
We strongly encourage contributions from racialized scholars and authors with lived experience or expertise in addressing systemic discrimination in health research.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being and SDG 10, Reduced Inequalities.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Aug 14, 2026
Health Inequities’ Lethal Impact
Advancing our collective understanding of health inequities remains essential for addressing the complex and often lethal consequences of systemic disparities in health outcomes. While significant progress has been made in recognizing the role of social determinants of health (SDOH), there is an urgent need to further investigate the structural injustices that perpetuate income inequality, racial and ethnic disparities, and the disproportionate burden of chronic disease—particularly among historically marginalized and underserved populations.
This Collection centers on the lethal impact of health inequities, with a primary focus on mortality and the systemic conditions that lead to preventable deaths. While morbidity—defined as the burden of disease and disability—plays a critical role in shaping health trajectories, it is the escalation to premature mortality that underscores the urgency of this research. Authors are strongly encouraged to examine how inequities contribute to death and life-shortening outcomes, rather than submitting work that addresses health equity in general without engaging with its fatal consequences.
Recent research has revealed that the relationship between morbidity and mortality is complex and non-linear. Some populations endure prolonged suffering due to chronic conditions, while others face abrupt and avoidable death due to systemic neglect. These patterns reflect the cumulative impact of adverse SDOH, such as housing insecurity, food instability, limited education, and lack of access to timely care.
Communities facing intergenerational trauma, persistent socioeconomic disadvantage, and discrimination—including Indigenous populations and other minoritized groups—are disproportionately affected. Individuals living in areas of high social vulnerability experience significantly higher all-cause mortality rates, and those with multiple concurrent adverse SDOH face the poorest health outcomes.
Ongoing examination of these issues is vital for informing evidence-based decision-making and equipping policymakers with the insights needed to foster equity in health. Beyond identifying policy failures, this Collection seeks to highlight mechanisms for translating research into equitable policy action. By bridging the gap between evidence and implementation, we aim to surface practical pathways for systemic change—whether through legislative reform, community-led initiatives, or integrated health system strategies.
We invite researchers to contribute to this special Collection, Health Inequities’ Lethal Impact. Topics of interest include, but are not limited to:
-Structural injustice and health
-The role of income inequality in health outcomes
-Racial and ethnic disparities in chronic disease
-Health inequities in Indigenous communities
-Policy interventions for reducing preventable deaths
-Mechanisms for translating evidence into equitable policy action
-Social determinants of health and morbidity
-Community-based approaches to health equity
-Examining policy failures in health systems
-Intersections of morbidity and mortality in vulnerable populations
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being and SDG 10, Reduced Inequalities, reinforcing the global imperative to ensure equitable access to health.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Nov 02, 2026

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in