From patients to tumor avatars: A journey towards personalized immunotherapy research
Published in Cancer

What drove us to develop a human 3D cancer model?
Immune checkpoint blockade targeting the PD-1/PD-L1 axis has transformed clinical cancer treatment in many tumor types. Therefore, it is rather surprising that relatively little is known on how tumors immunologically respond to this treatment. Mouse models have provided mechanistic insights into treatment responses, however translation of these observations to the variety of human cancers is challenging. Thus, we wanted to create a model that would allow us to study immunotherapy effects directly in human tissue. A major challenge of analyzing patient material is the difficulty to perform mechanistic studies. Our mission was to overcome this limitation by developing a fully human model that on one hand preserves the tumor microenvironment and architecture, and on the other hand can be perturbed by immunotherapeutic treatments. Towards this goal, our mentor and supervisor, Dr Daniela Thommen, had the idea to establish an ex vivo culture system using patient-derived tumor fragments (PDTFs) to dissect the early effects of PD-1 blockade across multiple cancer types.
Unique collaboration between bench and bedside
To develop our model, we had to address a number of challenges. First of all, we needed to obtain access to patient material. We are very fortunate to work in an exceptional institute such as the NKI-AVL, where hospital and research labs are under one roof and interactions between clinicians and researchers are common and frequent. We are particularly grateful to all the patients who were willing to donate their tumors for our research. Once we established the tumor material collection, the next challenge was to set up a logistic process that ensured to bring the material as fast as possible to the lab. For this, a close collaboration between clinicians, surgeons, pathologists and us researchers was needed. We installed a dedicated tumor collection team that is on stand-by to collect the tumor tissue as fast as possible after removal by the surgeon and bring it to the lab. We then immediately dissect the tissue into small fragments of 1-2 mm3 which we use for our cultures. To optimize the use of tumor material, we developed a cryopreservation protocol that allows us to store the tissue and phenotype each tumor before assigning it to a suitable project. Using this protocol, we have currently collected and stored patient material of over 370 tumors and 60,000 fragments in our biobank.
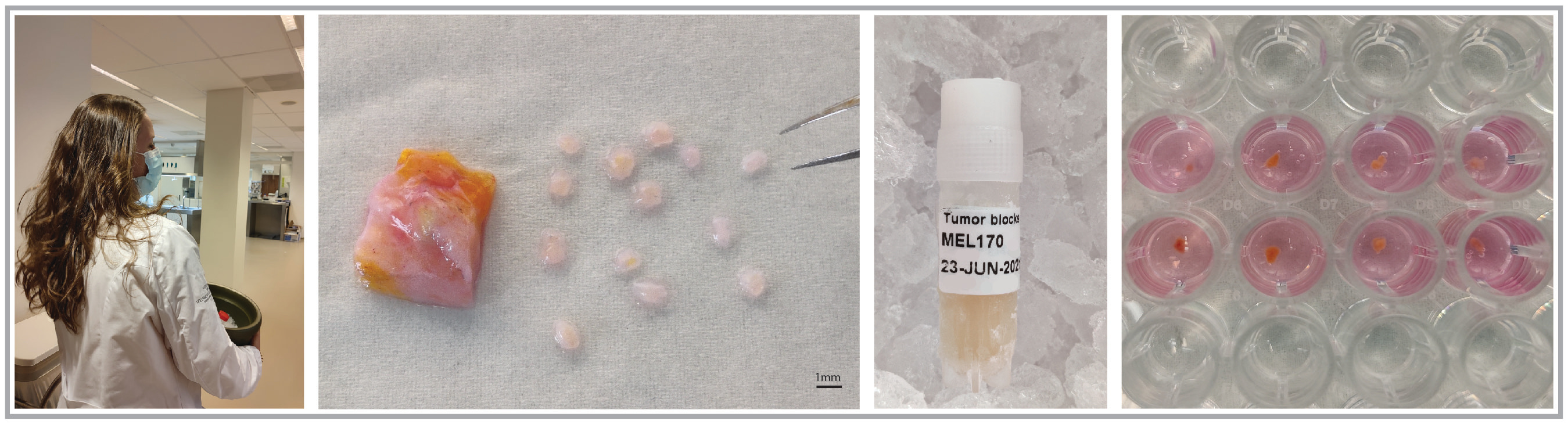
The 4-steps protocol from patients to bench. (From left to right) A member of our team (Marjolein de Bruijn) on stand-by to collect tumor tissue at Pathology. Right after at the laboratory, she dissects the tumor piece into small fragments of 1-2 mm3. Then the processed material is frozen and subsequently used in our culture system.
The PDTF platform as a model to dissect anti-PD-1 response
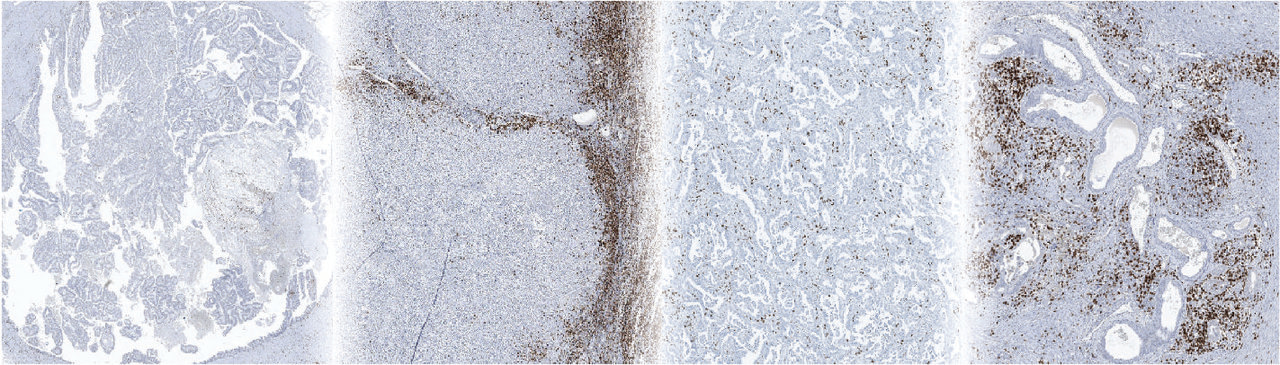
Our next step was to develop a culture system which can preserve the tumor tissue as close to the patient as possible. To this end, we established short-term cultures of 2 days which allow us to maintain a quite natural tumor microenvironment without the need to add any cytokines, growth factors or inhibitors. To validate our platform, we used PD-1 blockade as this would allow us to directly compare changes induced ex vivo with the clinical response of the patient. To this end, we treated tumor fragments from patients with five cancer types with anti-PD-1. Based on changes in multiple immune-related factors, we separated the tumors into responders and non-responders. The time to celebrate came some months later, when we discovered that 100% of the observed tumor tissue responses matched the clinical responses of the patients subsequently receiving anti-PD-1.
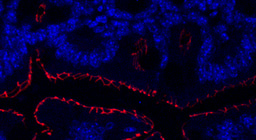
Now we could use the platform to dissect the observed immunological responses. By perturbing T cell activation and signaling pathways, we found that tumor-resident T cells were crucial to initiate these immunological responses and induced the secretion of multiple T cell chemoattractants in the tumor. These findings suggest a model in which PD-1 blockade may induce a local immune response in the tumor by reinvigorating tumor-resident T cells that subsequently promotes the recruitment of potentially more functional peripheral T cells, as observed in patients at later timepoints [1]. In addition, we identified baseline tumor properties associated with response or resistance to PD-1 blockade. Most interestingly and in line with earlier observations from our lab [2], we observed that the presence of a specific population of tumor-reactive T cells, so called PD-1T TILs, were highly predictive for response to PD-1 blockade. In addition, paralleling the predictive value established for clinical response [3-5], we found that the presence of tertiary lymphoid structures was also predictive for immunological response to anti-PD-1.
We believe that the PDTF platform is a powerful tool that could support the personalization of immunotherapy. One potential way to use the platform may involve a direct diagnostic application for immediate treatment decisions. However, a second, in our opinion more preferable, way is the use of the platform for the identification of new biomarkers and treatment options. A particular strength of the platform lies in the opportunity to compare different treatments side-by-side in the same tumor. In addition to its translational application, the PDTF platform is also a compelling tool for fundamental research, particularly as it allows combination with many other high-dimensional technologies, such as single cell RNA sequencing or spatial imaging methods, in a modular way.
As for many other labs, the COVID-19 outbreak has been a major challenge for our study, with the first lockdown fully interrupting patient sample collection for several months and the lab being almost completely closed. In the end, we are very grateful that we could succefully master all the above-mentioned challenges. Running this project really gave us an exceptional opportunity to get acquainted with the organizational aspects of large projects involving many different specialties. The entire journey brought us closer to the clinic and most importantly to the patients’ needs for a suitable and effective cancer treatment. We hope that the PDTF platform will be a tool for many to use and foster exciting discoveries in the future.
References
[1] Yost, K.E., et al. Clonal replacement of tumor-specific T cells following PD-1 blockade. Nature Medicine 25, 1251-1259 (2019).
[2] Thommen, D.S., et al. A transcriptionally and functionally distinct PD-1+CD8+ T cell pool with predictive potential in non-small cell lung cancer treated with PD-1 blockade. Nature Medicine 24, 994-1004 (2018).
[3] Cabrita, R., Lauss, M., et al. Tertiary lymphoid structures improve immunotherapy and survival in melanoma. Nature 577, 561-565 (2020).
[4] Helmink, B.A., Reddy, S.M., Gao, J., Zhang, S., Basar, R., et al. B cells and tertiary lymphoid structures promote immunotherapy response. Nature 577, 549-555 (2020).
[5] Petitprez, F., et al. B cells are associated with survival and immunotherapy response in sarcoma. Nature 577, 556–560 (2020).
Follow the Topic
-
Nature Medicine

This journal encompasses original research ranging from new concepts in human biology and disease pathogenesis to new therapeutic modalities and drug development, to all phases of clinical work, as well as innovative technologies aimed at improving human health.
Related Collections
With Collections, you can get published faster and increase your visibility.
Microbiome and energy metabolism
Publishing Model: Hybrid
Deadline: Dec 06, 2026
Digital Medicine for Infectious Diseases
Publishing Model: Hybrid
Deadline: Nov 09, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in