Gulf medical students and Food Dome dietary guidelines
Published in Healthcare & Nursing, Social Sciences, and Public Health
The Gulf region, home to some of the youngest populations in the region, is experiencing a rapid increase in overweight and obesity, particularly among students. Similar to global trends, students in the Gulf experience significant changes upon entering higher education, including emotional and psychosocial changes that directly impact their food choices and physical activity.
A number of studies have been conducted and published highlighting the importance of knowledge of dietary guidelines for promoting behavioral change aimed at reducing obesity and associated noncommunicable diseases. However, it should be noted that knowledge of the guidelines themselves does not necessarily mean adherence to them. On the other hand, it has been argued that such knowledge increases the likelihood that people will reconsider their dietary beliefs and preferences.
To prevent overnutrition, undernutrition, and micronutrient deficiencies, and to promote physical activity, the Arab Center for Nutrition developed the Food Dome Dietary Guidelines (FDDG) for the Middle East and North Africa (MENA) region. The Food Dome framework takes into account local habits, traditional food consumption patterns, and lifestyles and presents a set of evidence-based and theoretically supported dietary recommendations designed to promote healthy eating and regular physical activity, as well as combat obesity and obesity-related noncommunicable diseases in the MENA region. Given the high rates of obesity, particularly among students in the Gulf region, I studied the knowledge, attitudes, and behavior of medical students in relation to Food Dome.
Quantitative data analysis revealed that while just over half of the 414 respondents reported having heard of Food Dome, only a few participants (10.9%) correctly identified their recommendations. While one in seven reported following Food Dome recommendations, overall, across almost the entire sample, compliance with these recommendations was less than 40%.
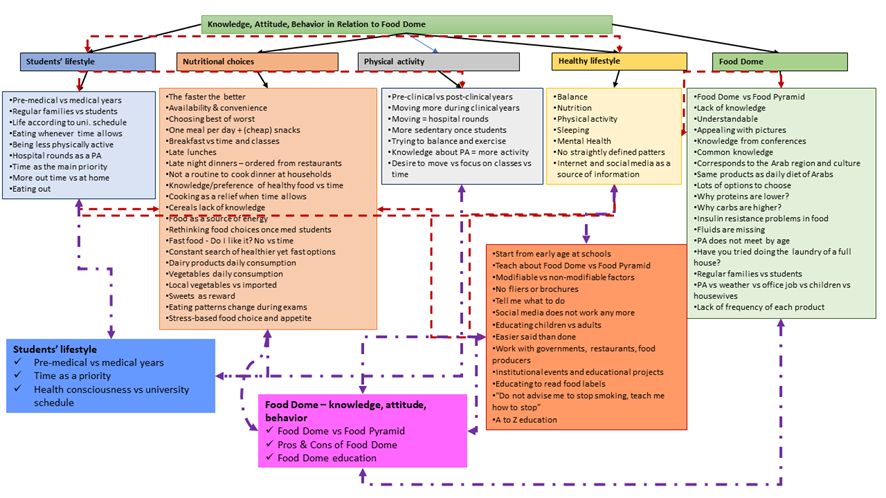
The qualitative phase of the research allowed me to immerse myself in the students' everyday lives, exploring the barriers and facilitators that support or hinder the adoption of healthy or unhealthy lifestyles in terms of nutrition and physical activity. There was a distinction of lifestyle between the pre-medical and medical periods. In their pre-medical years, most students ate at a specific time each day, exercised, and spent most of their time with their families. However, once they became students, their lives and the focus of their interests shifted to university: some made more conscious food choices and were more physically active, but most ate less healthily and were less active.
Although medical students from the Gulf states acknowledge the importance of healthy eating, physical activity, sleep, and other healthy lifestyle factors, their primary concern was aligning their day with the university schedule and meeting all assignment deadlines each semester. Most participants agreed that they increased their fast-food consumption due to busy schedules and lack of time to get home and have lunch with family. These findings are consistent with international data showing that the transition to higher education is a critical period for students in the Gulf, including changes in social contexts and the development of behavioral autonomy, which directly impacts their food choices. These patterns have been confirmed in previous studies among students from the United States, Brunei, Greece, and Germany.
Medical students from the Gulf region found the Food Dome to be clear, visually appealing, and conveying information through images. They also noted that it is common knowledge that food should not be distributed equally, but rather according to each person's needs. They believed that if the Food Dome, rather than the Food Pyramid, were introduced from an early age at their schools, food choices in adulthood would be much healthier. Additional suggestions included various events where healthcare facilities, schools, or restaurants could come together to discuss the dangers of unhealthy foods or recommended intake amounts for each food item, including nutritional information.
My mixed-methods research, allowed to suggest that the challenge of increasing food availability and changing attitudes toward healthy lifestyles and the Food Dome concept can be addressed through ongoing participatory research with local communities in the Gulf countries, enabling the development of policies best suited to the local environment and infrastructure. This endeavor should consider the various systems or contexts that shape human behavior, including the immediate environment in which a person resides, such as home, university, or workplace, as well as the relationships within and between these environments.
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in