HIV reservoir in tissue macrophages: from myth to reality
Published in Microbiology

Morgane Bomsel and Yonatan Ganor
Lab of Mucosal entry of HIV and mucosal immunity
Institut Cochin, CNRS UMR8104, INSERM U1016, Paris -France
morgane.bomsel@inserm.fr
Curing HIV-1-infected individuals of the virus is now a critical objective in the battle against HIV/AIDS. One major obstacle for HIV-1 eradication is the presence of a latent viral reservoir, a cell population in infected patients on combination antiretroviral therapy (cART) with undetectable plasma HIV-1 that produces infectious virus only following reactivation. Identification of all the diverse reservoirs that support viral persistence in patients on therapy is thus mandatory in the quest of a future HIV-1 cure.
Peripheral blood resting memory CD4+ T-cells remain the best-characterized HIV-1 reservoirs, but are probably not the only cell type in which HIV-1 can hide. Indeed, macrophages that possess specific features favorable for reservoir establishment might also harbor HIV-1 in virally suppressed HIV-1-infected patients. Hence, HIV-1-infected macrophages resist the cytopathic effects of viral infection and destruction by cytotoxic T-cells (CTLs), persist in tissues with a long half-life likely due to their self-renewing capacity, and produce and store infectious virus for extended periods of time in specific compartments, referred to as virus containing compartments (VCCs). Accordingly, it is known for several years that in HIV-1-infected and cART-suppressed individuals, residual viremia originates not only from T-cells but also from macrophages. As an additional indication of the capacity of macrophages to act as HIV-1 reservoirs, Garcia’s group recently established that macrophages sustained HIV-1 replication in vivo in humanized mice reconstituted only with macrophages and lacking T-cells. When these animals were virally suppressed with ART, viral rebound was observed upon ART interruption. However, this simplified macrophage-only humanized mouse model does not fully recapitulate the human immune system with its variety of potential HIV-1 target cells. Although additional studies by DiNapoli et al in monkeys reported the presence of HIV-1 components in various tissue macrophages, replication-competent viruses could not be detected in this study.
It is important to remember that HIV-1 is mainly a sexually transmitted infection occurring especially at the genital and rectal mucosa. More than 60 million people are infected to date, approximately half of which are men. The adult human penis is the most likely HIV-1 entry site in heterosexual men, and in men having sex with men (MSM), penile infection accounts for a third of infection cases. For many years, the study of HIV-1 entry in the male genitals lagged over that in the female and gastrointestinal tracts, most probably due to the difficulty in obtaining relevant tissues. Nevertheless, we recently identified the inner foreskin in non-circumcised men and the penile urethra as primary entry sites for HIV-1 in men upon unprotected sexual intercourses. At each site, different immune cells are targeted by HIV-1, namely Langerhans cells in the inner foreskin and macrophages in the urethra.
Thus, to get a full picture of the HIV-1 reservoir landscape and set the stage for the development of future and efficient HIV-1 purging strategies, it was crucial to determine if macrophages could form genuine reservoirs in mucosal and especially genital tissues, and determined their capacity to be reactivated and produce infectious virus.
We got very excited when we could access penile tissues from men -undergoing gender reassignment-, not only from healthy individuals to recapitulate penile infection ex vivo as we had done before, but also from HIV-infected and cART-suppressed individuals. And more than two dozens of such tissues! Just enough to search for the presence of HIV-1 components in their urethral macrophage but also to evaluate the capacity of these cells to produce infectious viruses upon specific reactivation ex-vivo, the definitive criteria identifying an HIV-1 reservoir.
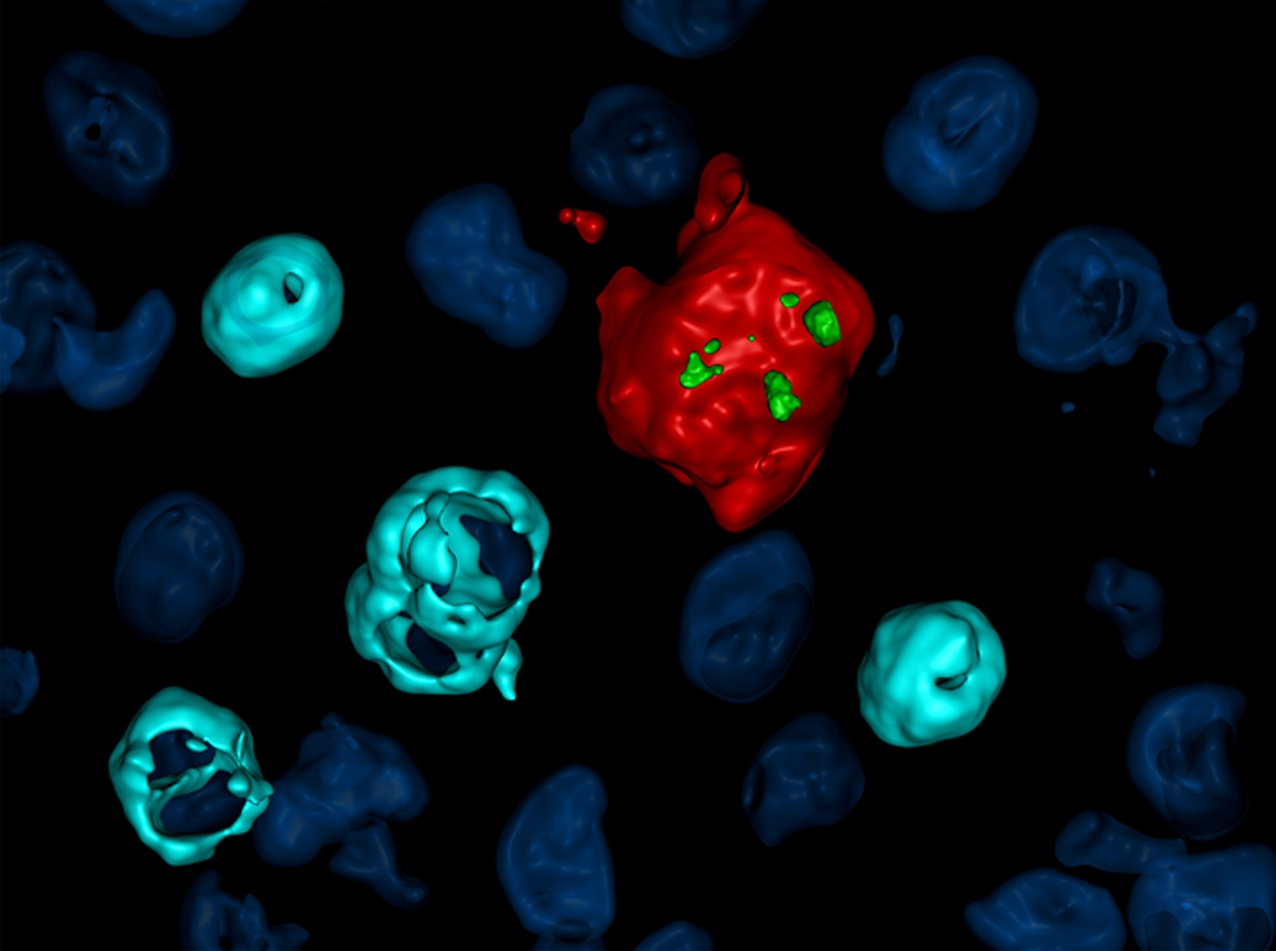
By using a combination of different approaches, our study is the first to show that in human, tissue macrophages form a reservoir for HIV-1 in infected patients under suppressive cART. Such macrophage reservoirs not only contain integrated HIV-1 DNA, RNA and viruses in intracellular VCC-like structures, but also can produce infectious HIV-1 upon macrophage-specific reactivation by LPS through the Toll-like receptor 4 (TLR-4), an innate immunity receptor. And to our surprise, we could not detect either virus or viral components in mucosal urethral T-cells in these patients. Urethral macrophages were the selective HIV-1 reservoirs, not urethral T-cells!
In addition, we show that in situ, within these mucosal tissues from HIV-1-infected and cART-suppressed patients, CTLs form conjugates with latently infected macrophages in a microenvironment rich in IFNg, which might render macrophages killing inefficient and sustain persistence of HIV-1 reservoirs in urethral macrophages, as very recently suggested from in vitro experiments by Clayton et al.
Furthermore, our study identifies a new subset of polarized urethral macrophages, expressing simultaneously markers of both the M1 and M2 polarization extremes, namely IL-4R, CD206 and IL-1R. Markedly, the HIV-1 reservoir pool is predominantly established in this newly identified intermediate macrophage subset, which is significantly increased in HIV-1-infected cART-suppressed compared to normal urethra.
Altogether, our results indicate that in human genital tissues, a replication-competent HIV-1 reservoir form in a new subset of macrophages. These findings call for a change of the “T-cell-only reservoir” paradigm. This more accurate understanding of HIV-1 persistence despite cART in men opens the door to the design of novel and better-adapted antiviral strategies. Such new strategies should definitely consider purging HIV-1 also from reservoirs in macrophages, in order to achieve the clinical goal of HIV-1 eradication. Of course, many questions remain: are these macrophage reservoirs fully latent or replicating at very low level, similar to T-cell reservoirs as recently described, thereby sustaining local inflammation? Do these macrophage reservoirs shed HIV-1 into semen once reactivated during bacterial infections? Can TLR-4 signaling pathway and clinically approved TLR-4 agonists be exploited to reactivate macrophage reservoirs in “shock and kill” strategies aimed at eradicating the virus? What is the precise origin of these macrophage reservoirs?
The myth of HIV-1 reservoirs in tissue macrophages becomes now a reality and only the tip of the iceberg was revealed. The story is just beginning.
Follow the Topic
-
Nature Microbiology
An online-only monthly journal interested in all aspects of microorganisms, be it their evolution, physiology and cell biology; their interactions with each other, with a host or with an environment; or their societal significance.





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in