How amygdala plays in obsessive-compulsive disorder: Magnetic resonance imaging reveals a specific role of amygdala subregions
Published in Healthcare & Nursing
Although many people experience minor obsessions (such as worrying about leaving the gas on, or if the door is locked) and compulsions (such as avoiding the cracks in the pavement), these do not typically impair interpersonal and occupational function. Obsessive-compulsive disorder (OCD) is a highly prevalent and chronic mental disorder characterized by the presence of severe obsessions and/or compulsions1. Obsessions are intrusive and persistent thoughts, images, impulses or urges, and are commonly associated with anxiety. Compulsions are repetitive behaviors or mental acts that the individual feels compelled to perform with the hope to mitigate the distress caused by obsessions, or to achieve a sense of completeness. The repetitive behaviors, such as washing/cleaning, ordering/counting, checking or other activities, can severely interfere with daily life. Most OCD patients are keenly aware that their symptoms are unwanted and excessive but just can’t disengage from the obsessive thoughts or stop the compulsive actions.
Neuroscientists are still uncertain about what happens in the brain to cause OCD, but one popular hypothesis points to the involvement of cortico-striato-thalamo-cortical (CSTC) circuits2. The general organizing theme of these circuits is that they project from specific territories in frontal cortex, to corresponding targets within striatum, and then via direct or indirect pathways through the basal ganglia to the thalamus, and finally with recurrent projections back to the original frontal territory where each loop started. This model of OCD is supported by a confluence of evidence from studies of brain imaging, cognitive-affective neuroscience, neuromodulation, and animal models. More recent research, however, suggests that this model is insufficient3,4.
The classical CSTC model does not take into consideration the essential role of amygdala and its interaction with the frontal cortex in mediating fear and anxiety in patients with OCD. Amygdala-based network dysfunction has been recognized as an updated model underlie the pathophysiology and symptomatology of OCD. Within this model, the amygdala is hyper-responsive to fear and uncertainty and lacks optimal functional interactions with prefrontal regions, leading to production and/or maintenance of fear in the context of OCD triggers.
The emergence of functional magnetic resonance imaging provides a possibility to non-invasively outline brain connectivity at rest, which greatly contributes to our understanding of the neurocircuitry models of various mental disorders. Seed-based functional connectivity (SBFC) analysis is one of the most popular tool to characterize the functional architecture of spontaneously coupled brain connectivity in mental disorders5. Only three studies to date have investigated the alterations of amygdala functional connectivity in OCD patients compared with healthy controls (HC) using whole-brain SBFC approach with two studies failing to find any significant differences between OCD patients and HC6,7. The only one demonstrated decreased intrinsic connectivity between the right amygdala and the right postcentral gyrus in medicated OCD patients8. Nevertheless, all these studies have examined the amygdala as a single, homogeneous region, disregarding the separable functions and connectivity profiles of its distinct subregions.
In our paper “Disorganized functional architecture of amygdala subregional networks in obsessive-compulsive disorder” published in Communications Biology, we applied connectivity-based parcellation to segment the amygdala to characterize functional architecture of amygdala-centered subtle networks in OCD patients. Capitalizing on the distinct connectivity pattern of each area, connectivity-based parcellation divides a region of interest (ROI) into distinct subregions9. The key idea is to first compute connectivity pattern for each individual voxel in the ROI, then use clustering algorithm to group the ROI voxels such that connectivity pattern is similar for the voxels within a group and different between groups, and finally identify distinct clusters in the ROI.
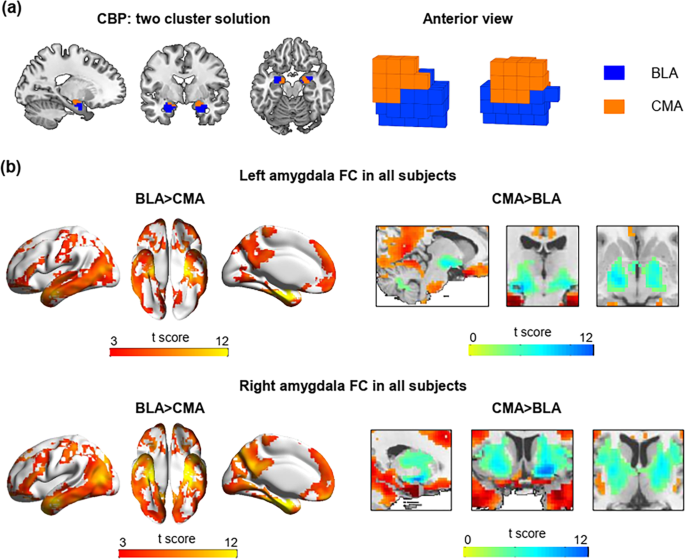
Connectivity-based parcellation derived subregions can achieve better performance in terms of resting-state signal homogeneity and provide a good representation of our specific sample for subsequent functional connectivity analyses. Using this connectivity-based framework with clustering algorithms, we segment the amygdala into basolateral amygdala (BLA) and centromedial amygdala (CMA), each of which exhibited preferential functional connectivity with specialized brain regions (see Figure 1).
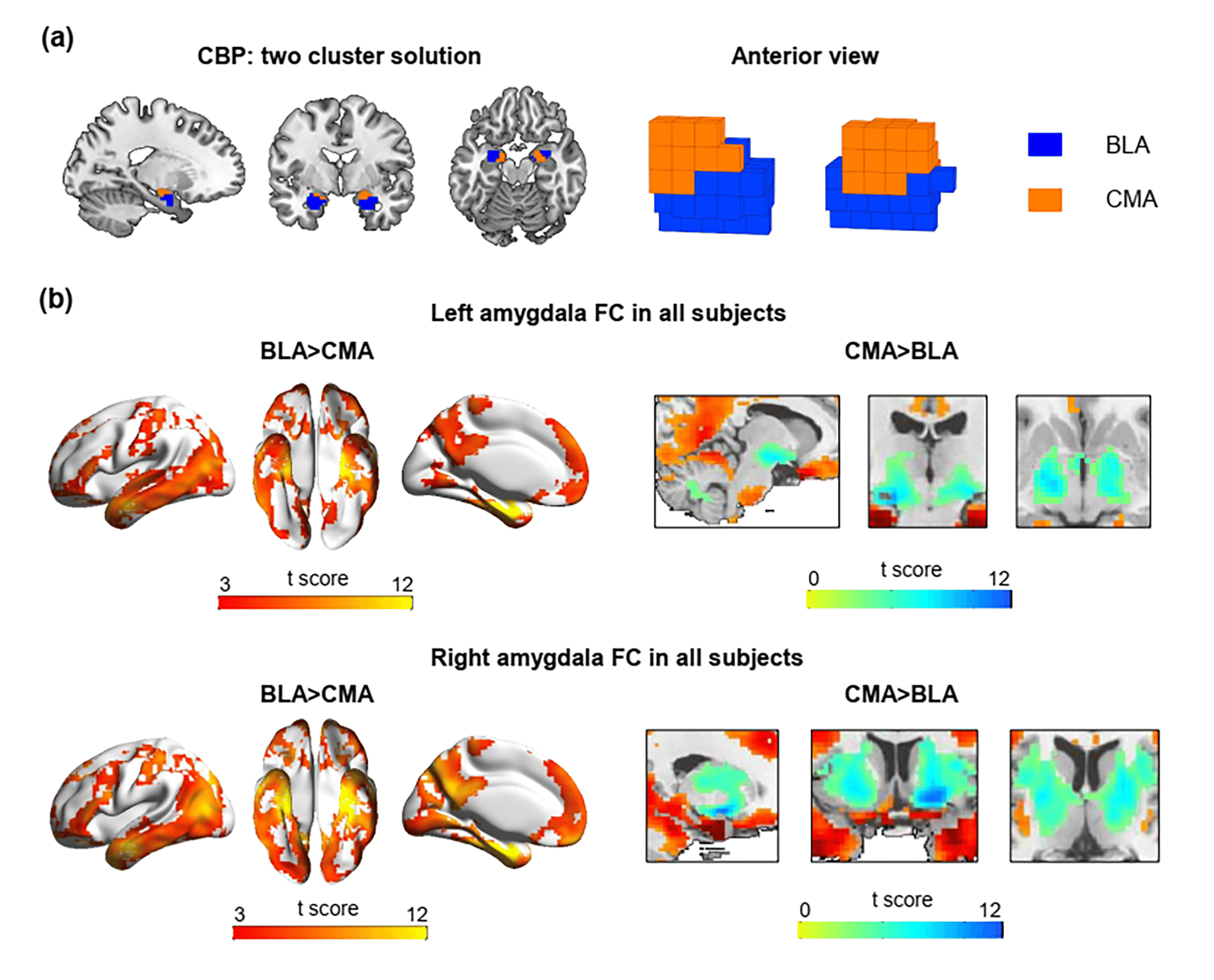
Figure 1 Connectivity-based parcellation of the amygdala. (a) The two-cluster solution derived by connectivity-based parcellation (CBP). (b) The basolateral cluster (BLA) connectivity was primarily cortical, whereas the centromedial cluster (CMA) connectivity was primarily subcortical. Warm color (red) indicates that BLA connectivity is stronger compared to CMA connectivity whereas cool color (blue) indicates CMA connectivity is stronger compared to BLA connectivity.
Overall, we found OCD patients demonstrated disorganized patterns of differentiated BLA-CMA functional connectivity, specifically with several brain regions including insula, supplementary motor area (SMA), midcingulate cortex (MCC), superior temporal gyrus (STG) and postcentral gyrus (PCG). HC group exhibited stronger BLA connectivity with these regions compared to CMA, whereas in OCD patients, the connectivity pattern reversed to stronger CMA connectivity comparing to BLA. Further analyses revealed such disruption in OCD patients were driven by hypoconnectivity between left BLA and left insula, and hyperconnectivity between right CMA and bilateral SMA, MCC, STG, PCG, and right insula. (see Figure 2)
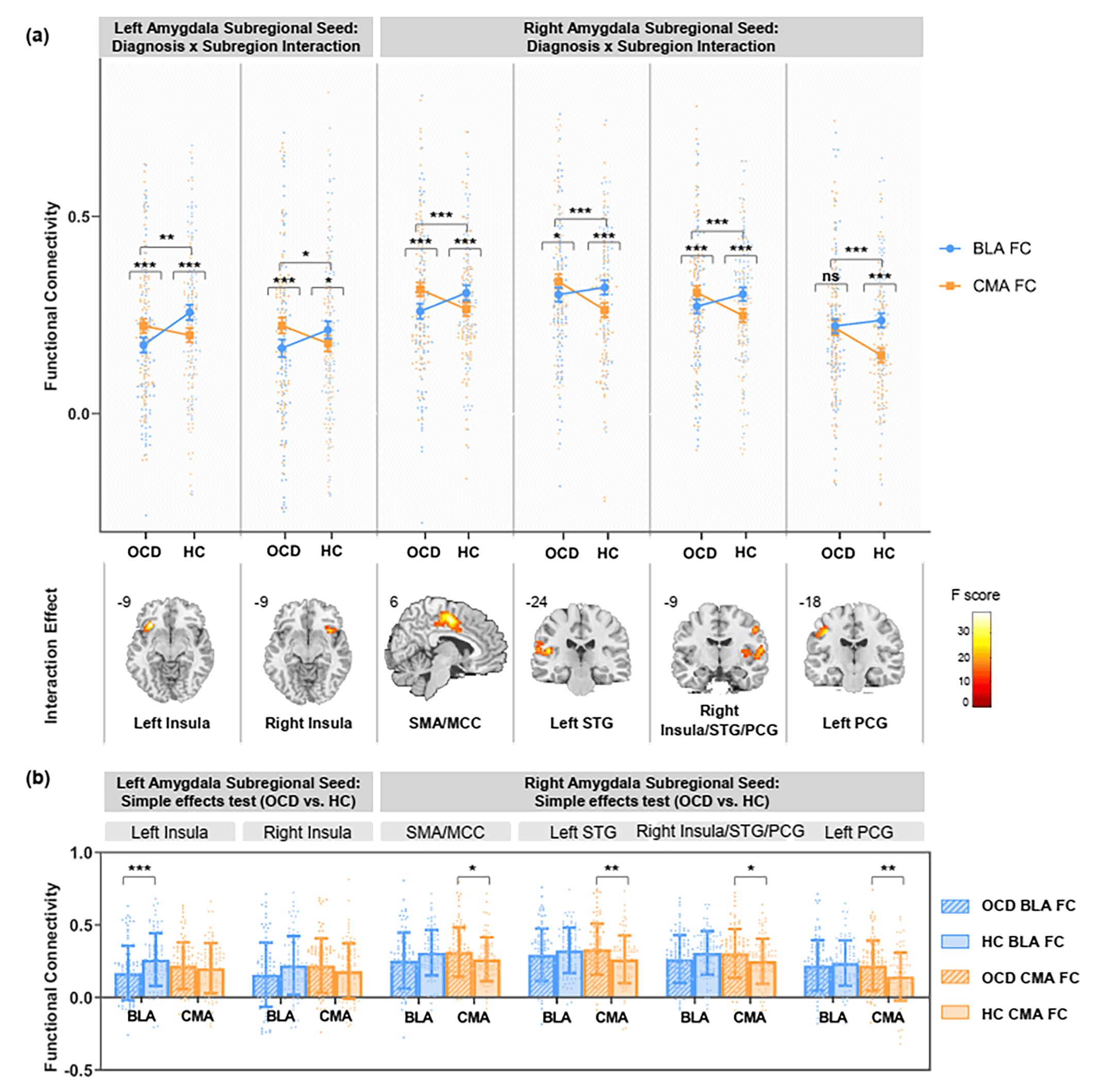
Figure 2 Amygdala subregional functional connectivity in OCD and HC. (a) Significant interactions between diagnosis (OCD vs. HC) and subregion (BLA vs. CMA) computed separately in left and right amygdala. Error bars represent standard errors of the means. (b) Simple effects tests comparing functional connectivity (FC) between OCD versus HC in each subregion. Significance is indicated for uncorrected *p<.05; **p<.01; ***, p<.005. Error bars represent standard deviation. n=182 biologically independent samples were used to derive statistics. MCC, midcingulate cortex; PCG, postcentral gyrus; SMA, supplementary motor area; STG, superior temporal gyrus.
We additionally extracted the volume of amygdala subregions to determine whether functional aberrations were accompanied by structural changes. Structural analyses revealed reduced volume of the bilateral BLA and right CMA subnuclei in OCD patients compared with HC. Since network communication depend heavily on structural properties of neuronal cells (e.g., size, configuration, and arrangement), we tentatively hypothesized that amygdala subregional network dysfunction in OCD is related to structural defects. However, the exact mechanism about how the change in structure impact human brain function is still poorly understood. Future advances in imaging technology, and greater dialogue between human neuroimaging studies and cellular/molecular neuroscience, could further our understanding of the complicated structure-function relationship.
References
1 Stein, D. J. et al. Obsessive-compulsive disorder. Nat Rev Dis Primers 5, 52, doi:10.1038/s41572-019-0102-3 (2019).
2 Goodman, W. K., Storch, E. A. & Sheth, S. A. Harmonizing the Neurobiology and Treatment of Obsessive-Compulsive Disorder. Am J Psychiatry 178, 17-29, doi:10.1176/appi.ajp.2020.20111601 (2021).
3 Milad, M. R. & Rauch, S. L. Obsessive-compulsive disorder: beyond segregated cortico-striatal pathways. Trends Cogn Sci 16, 43-51, doi:10.1016/j.tics.2011.11.003 (2012).
4 Shephard, E. et al. Toward a neurocircuit-based taxonomy to guide treatment of obsessive-compulsive disorder. Mol Psychiatry 26, 4583-4604, doi:10.1038/s41380-020-01007-8 (2021).
5 Woodward, N. D. & Cascio, C. J. Resting-State Functional Connectivity in Psychiatric Disorders. JAMA Psychiatry 72, 743-744, doi:10.1001/jamapsychiatry.2015.0484 (2015).
6 Paul, S. et al. Amygdala-prefrontal connectivity during appraisal of symptom-related stimuli in obsessive-compulsive disorder. Psychol Med 49, 278-286, doi:10.1017/s003329171800079x (2019).
7 Sha, Z. Q. et al. Functional disruption in prefrontal-striatal network in obsessive-compulsive disorder. Psychiatry Research-Neuroimaging 300, doi:10.1016/j.pscychresns.2020.111081 (2020).
8 Picó-Pérez, M. et al. Intrinsic functional and structural connectivity of emotion regulation networks in obsessive-compulsive disorder. Depress Anxiety 36, 110-120, doi:10.1002/da.22845 (2019).
9 Eickhoff, S. B., Thirion, B., Varoquaux, G. & Bzdok, D. Connectivity-based parcellation: Critique and implications. Hum Brain Mapp 36, 4771-4792, doi:10.1002/hbm.22933 (2015).
Follow the Topic
-
Communications Biology
An open access journal from Nature Portfolio publishing high-quality research, reviews and commentary in all areas of the biological sciences, representing significant advances and bringing new biological insight to a specialized area of research.

Related Collections
With Collections, you can get published faster and increase your visibility.
From RNA Detection to Molecular Mechanisms
Publishing Model: Open Access
Deadline: May 05, 2026
Advances in neurodegenerative diseases
Publishing Model: Hybrid
Deadline: Jun 30, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in