Lymphatic filariasis setbacks after COVID-19
Published in Microbiology and General & Internal Medicine

Lymphatic filariasis (LF), commonly known as elephantiasis, is one of the world’s most neglected tropical diseases (NTDs). Considered one of the ‘big five’ NTDs, it affects hundreds of millions of people worldwide, largely in low-income tropical regions.
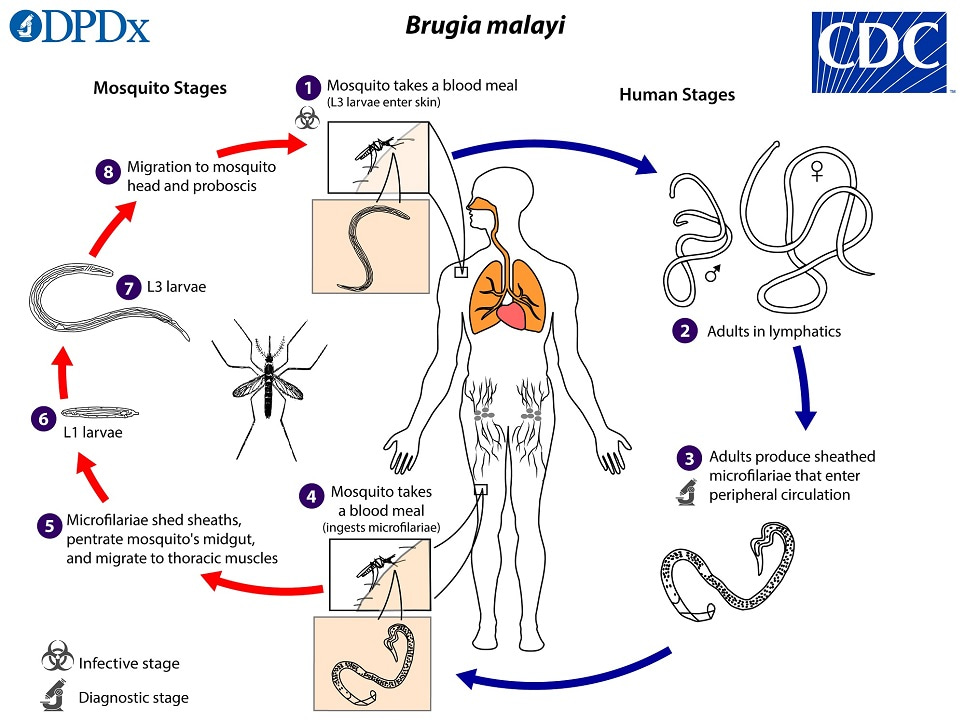
The disease is primarily caused by three parasitic nematodes, Wuchereria bancrofti, Brugia malayi, and B. timori, which are transmitted by a range of mosquito species depending on the nematode species and the geographical location.
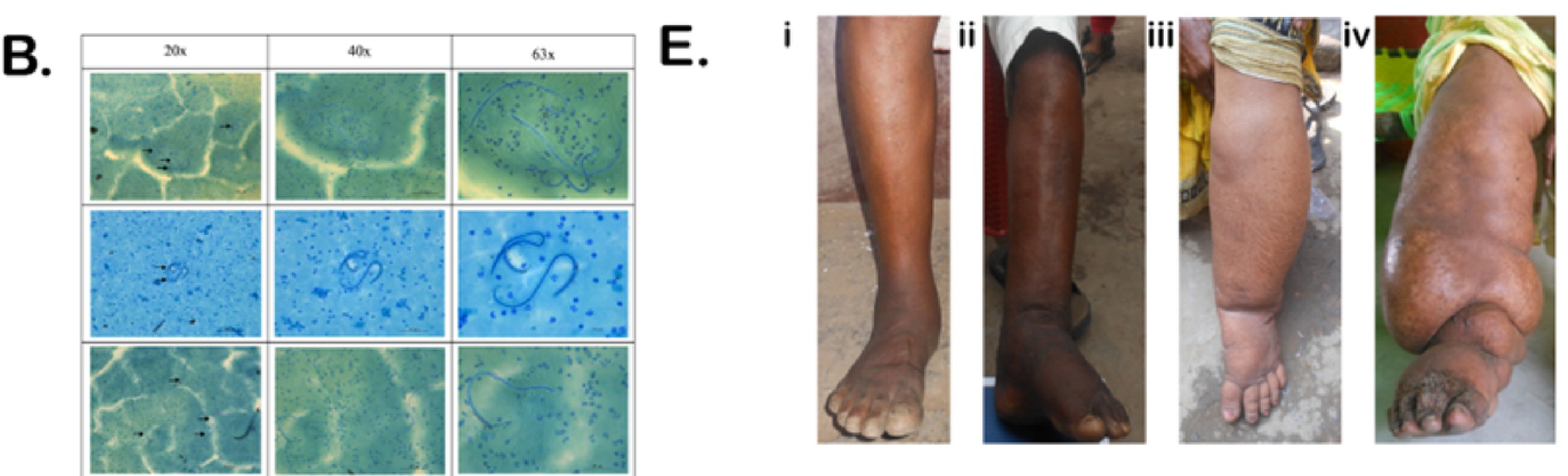
The infection causes disruption and damage to the lymphatic system, which can lead to dramatic and disfiguring swelling of limbs and genitals. Although these visible symptoms typically emerge later in life, infection is usually acquired in childhood, silently progressing for years. For many, the consequences extend far beyond physical illness, with disability, stigma, and loss of income all contributing to a cycle of poverty that disproportionately affects already vulnerable communities.
Encouragingly, global control efforts have led to substantial declines in disease burden. Since 2000, more than 9.7 billion treatments have been delivered through mass drug administration (MDA), contributing to a 74% reduction in infections. However, these gains are rather fragile, relying on sustained public health interventions and consistent community engagement. What happens when these efforts are interrupted, as many NTD treatment programmes were during the and after the COVID-19 pandemic?
Tracking filariasis through disruption
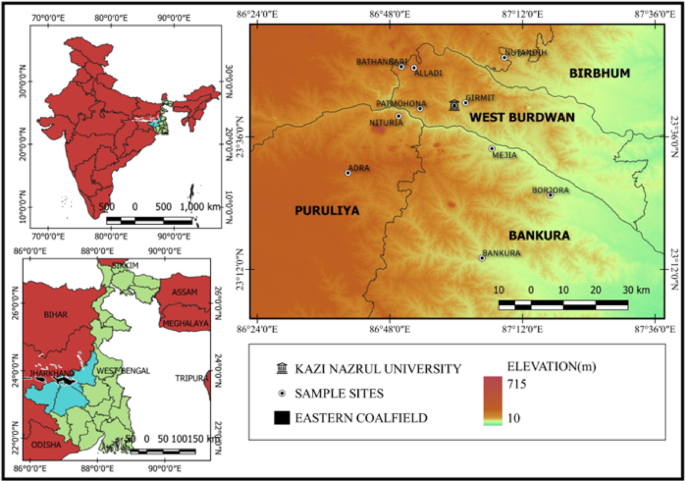
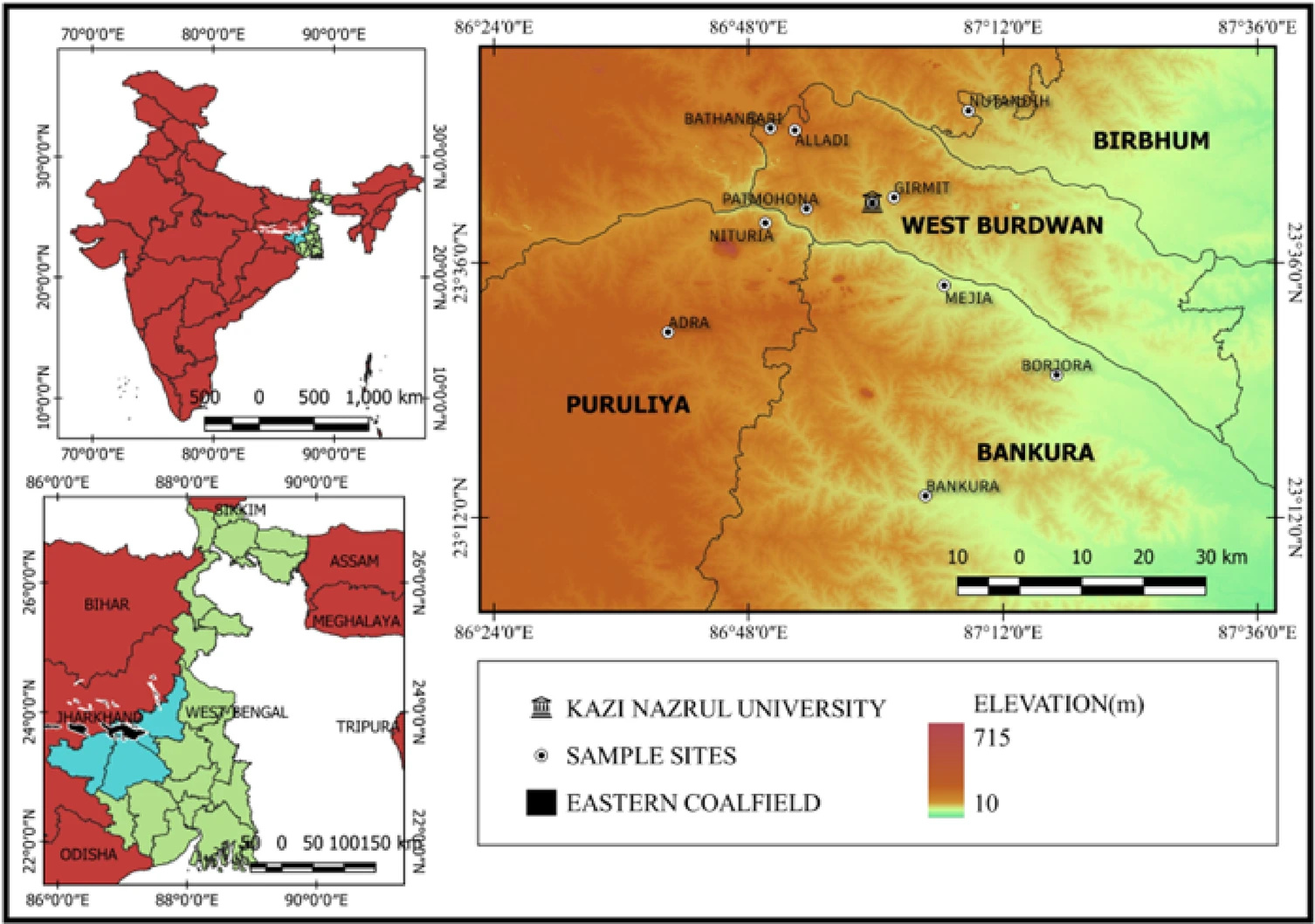
A recent study by Chakraborty and colleagues provides an insight into LF in a high-risk setting, where the team investigated the prevalence and health burden of bancroftian filariasis (caused by W. bancrofti) in the eastern coalfield regions of West Bengal in India, an area that has historically been under-surveyed.
Crucially, the study spans the period during and after the COVID-19 pandemic, offering an opportunity to examine how disruptions to public health programmes may have influenced disease dynamics.
By combining large-scale community screening and clinical assessments, the researchers set out to measure how widespread infection currently is, to understand who is most affected, how severe the disease has become, and how it intersects with other health conditions.
An unforeseen setback
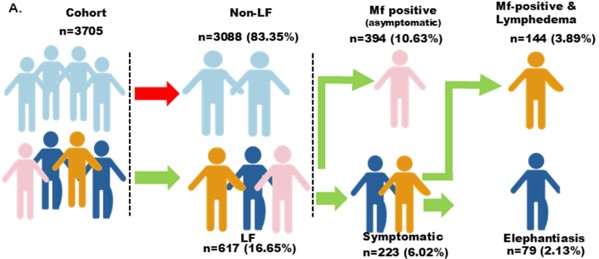
From surveys and clinical assessments of 3,705 individuals conducted between 2021 and 2024, the researchers found an overall LF prevalence of 16.65%, with 14.5% showing active infection. This is substantially higher than earlier reports from the same region, which had suggested much lower levels in some districts, some below 1%.
Breaking down these infections, around two-thirds of cases were asymptomatic, meaning infected individuals showed no obvious signs but still carried the parasite and could contribute to transmission. The remaining cases included people with clinical disease, many with moderate to severe lymphedema.
The identification of a large, largely invisible reservoir of asymptomatic infection quietly sustaining transmission, is of considerable concern. The authors suggest that the interruption of MDA campaigns and disrupted routine healthcare services due to COVID-19 likely allowed transmission to persist, or even rebound. At the same time, reduced access to care may have worsened outcomes for those already living with the disease.
More than a parasitic infection
A high burden of comorbidities among affected populations were also identified in the study, including hypertension, obesity, cardiovascular disease, and fungal infections. For example, fungal infections were found to be strongly associated with severe lymphedema, likely due to impaired lymphatic function and skin damage.
As with many diseases, complex interactions between conditions can significantly worsen disease symptoms and progression, and here, it reinforces the idea that LF is not an isolated or obscure parasitic disease, but part of a broader web of health challenges shaped by poverty, environment, and access to care.
What does this mean for elimination efforts?
Globally, LF elimination programmes aim to stop transmission while also managing long-term disability. The presence of many asymptomatic carriers here indicates that transmission is ongoing, while the high number of chronic cases highlights gaps in morbidity management and disability prevention. Importantly, the findings show how quickly progress can stall when health systems are disrupted for even a relatively short time.
For LF, the path to elimination remains achievable, but it will require renewed commitment, especially in underserved and high-risk communities like those in the Eastern Coalfield districts of West Bengal. The authors argue for a renewed approach with strengthened MDA campaigns, improved access to basic care and hygiene interventions, and addressing comorbid conditions alongside LF itself.
Dr. Daniel Parsons is a bioinformatician and post-doctoral researcher at the Natural History Museum, London.
His research has largely focused on improving understanding of parasitic flatworm biology and genetic variability, notably schistosomes (causative agents of schistosomiasis), through the application of molecular techniques and genomics approaches. More broadly, Dan is interested in the applications of biotechnology for Neglected Tropical Disease research and how biodiversity and global health are interlinked.
Follow the Topic
-
Scientific Reports
An open access journal publishing original research from across all areas of the natural sciences, psychology, medicine and engineering.
-
BugBitten
A blog for the parasitology and vector biology community.


Related Collections
With Collections, you can get published faster and increase your visibility.
Computational biology and mathematical modelling of biological systems
Publishing Model: Open Access
Deadline: Jul 18, 2026
Water pollution and advanced treatment processes
Publishing Model: Hybrid
Deadline: May 31, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in