Opioid misuse in patients with cancer
Published in Cancer, General & Internal Medicine, and Pharmacy & Pharmacology

Opioids are ancient drugs. Their euphoric, relaxing, and analgesic effects have been described in the history since Sumerian and Egyptian civilizations. They were included in the analgesic ladder for cancer pain treatment proposed by the World Health Organization in 1986 and remain as gold standard for the management of severe/moderate cancer pain.1,2 In recent decades, the evidence regarding the successful analgesic effects of opioids for cancer pain supported the transference of knowledge to apply the same treatment principles to chronic non-cancer pain. Subsequently, prescribed opioid consumption increased worldwide. However, the doubts regarding positive effects of long-term opioid administration on chronic non-cancer pain and reports of neurotoxicity and iatrogenic consequences as opioid misuse have raised red flags. A notorious example is the USA, which for decades have faced an opioid crisis characterized by the indiscriminate escalation of prescribed opioids, misuse problems, and overdose-related deaths. Observing how opioids can have disastrous consequences in patients with chronic non-cancer pain, it has been hypothesized that this may also happen in patients with cancer in opioid treatment. Particularly, because the scene of cancer pain treatment in general has changed dramatically in recent years.
In the 1990s, there was a prevailing belief that opioid use for cancer pain carried a minimal risk of addiction of less than 1%. Some factors, such as the severity of the disease, shorter life expectancy and opioid use in late stages of the disease trajectory, possibly mitigated the significance of opioid misuse and addiction for this population. However, knowledge has evolved. Advances in diagnostics and antineoplastic treatments have improved prognosis and increased survival rates in the majority of patients with cancer.3 Survivors or patients with chronic disease may suffer the consequences of the disease and treatment and among others end up with chronic pain.4 Further, in high income countries a movement towards integration of palliative care and oncology is on the agenda, which promotes earlier palliative care interventions including the use of opioids throughout the cancer journey.5 Thus, it seems like patients with cancer treated with opioids for long periods may continue with opioid treatment after recovering from cancer. This new aspect in the cancer pain treatment is little explored but deserves careful attention.
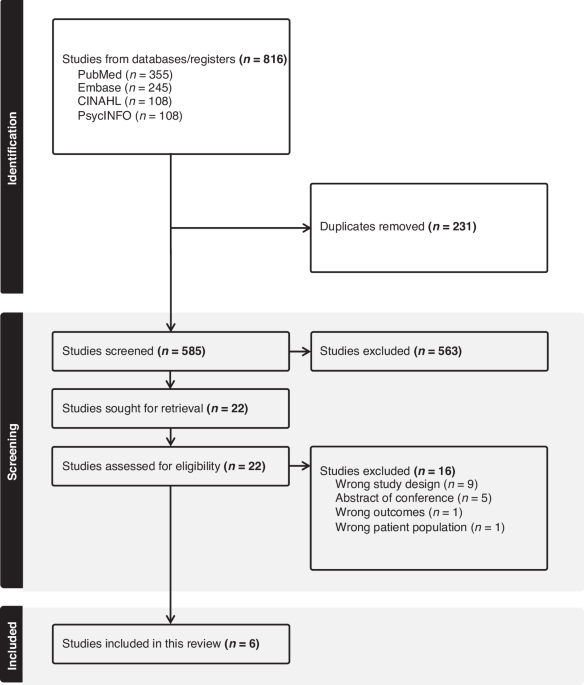
Our research group examined the scientific evidence regarding opioid misuse in patients with cancer in long-term opioid treatment. Applying the definition that opioid misuse is the use of prescription opioids in a different manner than as directed by a doctor6, we found very few prospective studies on the subject (n=6). It was quite overwhelming to learn that the prevalence of actual opioid misuse in patients with cancer varied between 5.7% and 84% and the risk of opioid misuse between 2.4% to 35.4% (pooled prevalence of opioid misuse risk =12.3%). Thus, opioid misuse in cancer seems to be more frequent than previously believed.
Unfortunately, the fear of addiction has been one of the barriers to using opioids for treating patients with cancer pain in several clinical settings around the world7. The combination of this fear with other factors often prevents patients with cancer pain from receiving adequate pain treatment. Opioid guidelines have been developed to guide clinicians and improve cancer pain management. Recent guidelines have also included information about the risk of opioid addiction/misuse8,9, but recommendations to minimize and solve the problem are few and based on low levels of evidence, which demonstrate the need for more investigations. The demand for expertise to prevent, assess and treat opioid misuse tends to increase as the awareness of this issue grows. The future will require more efforts on preventive measures, education of healthcare professionals and patients, innovation in pain management, investment in treatment of opioid use disorders, strict regulation on opioid prescribing/monitoring and public health policy.
In a global perspective, we should have in mind that in most high-income countries opioids are readily accessible, but are consequently also subject to risk of overuse and misuse. However, cancer pain management is still far from perfect. On the other hand, many low-income countries have limited access to licensed opioid drugs and patients struggle for better pain management.
Geana Paula Kurita
Rigshospitalet Copenhagen University Hospital, University of Copenhagen
Per Sjøgren
Rigshospitalet Copenhagen University Hospital
References
- World Health Organization (WHO). WHO guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents. 2018. https://www.who.int/publications/i/item/9789241550390
- Ventafridda V, Tamburini M, Caraceni A, De Conno F, Naldi F. A validation study of the WHO method for cancer pain relief. Cancer. 1987 Feb 15;59(4):850-6.
- Miller KD, Nogueira L, Devasia T, Mariotto AB, Yabroff KR, Jemal A,et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022 Sep;72(5):409-436. doi: 10.3322/caac.21731. Epub 2022 Jun 23. PMID: 35736631.
- Snijders RAH, Brom L, Theunissen M, van den Beuken-van Everdingen MHJ. Update on Prevalence of Pain in Patients with Cancer 2022: A Systematic Literature Review and Meta-Analysis. Cancers (Basel). 2023 Jan 18;15(3):591.
- Kaasa S, Loge JH, Aapro M, Albreht T, Anderson R, Bruera E, et al. Integration of oncology and palliative care: a Lancet Oncology Commission. Lancet Oncol. 2018 Nov;19(11):e588-e653.
- National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services. Prescription opioids drugfacts. [cited 2023 Oct 20]. Available from: https://nida.nih.gov/publications/drugfacts/prescription-opioids
- Silbermann M, Calimag MM, Eisenberg E, Futerman B, Fernandez-Ortega P, Oliver A, et al. Evaluating Pain Management Practices for Cancer Patients among Health Professionals: A Global Survey. J Palliat Med. 2022 Aug;25(8):1243-1248.
- Paice JA, Bohlke K, Barton D, Craig DS, El-Jawahri A, Hershman DL, et al. Use of opioids for adults with pain from cancer or cancer Treatment: ASCO Guideline. J Clin Oncol. 2023 Feb 1;41(4):914-930.
- Swarm RA, Paice JA, Anghelescu DL, Are M, Bruce JY, Buga S, et al. Adult Cancer Pain, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019 Aug 1;17(8):977-1007.
Follow the Topic
-
British Journal of Cancer

This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in