The relevance of T helper cells that are induced by a mutant IDH1 vaccine in newly diagnosed astrocytoma
Published in Cancer
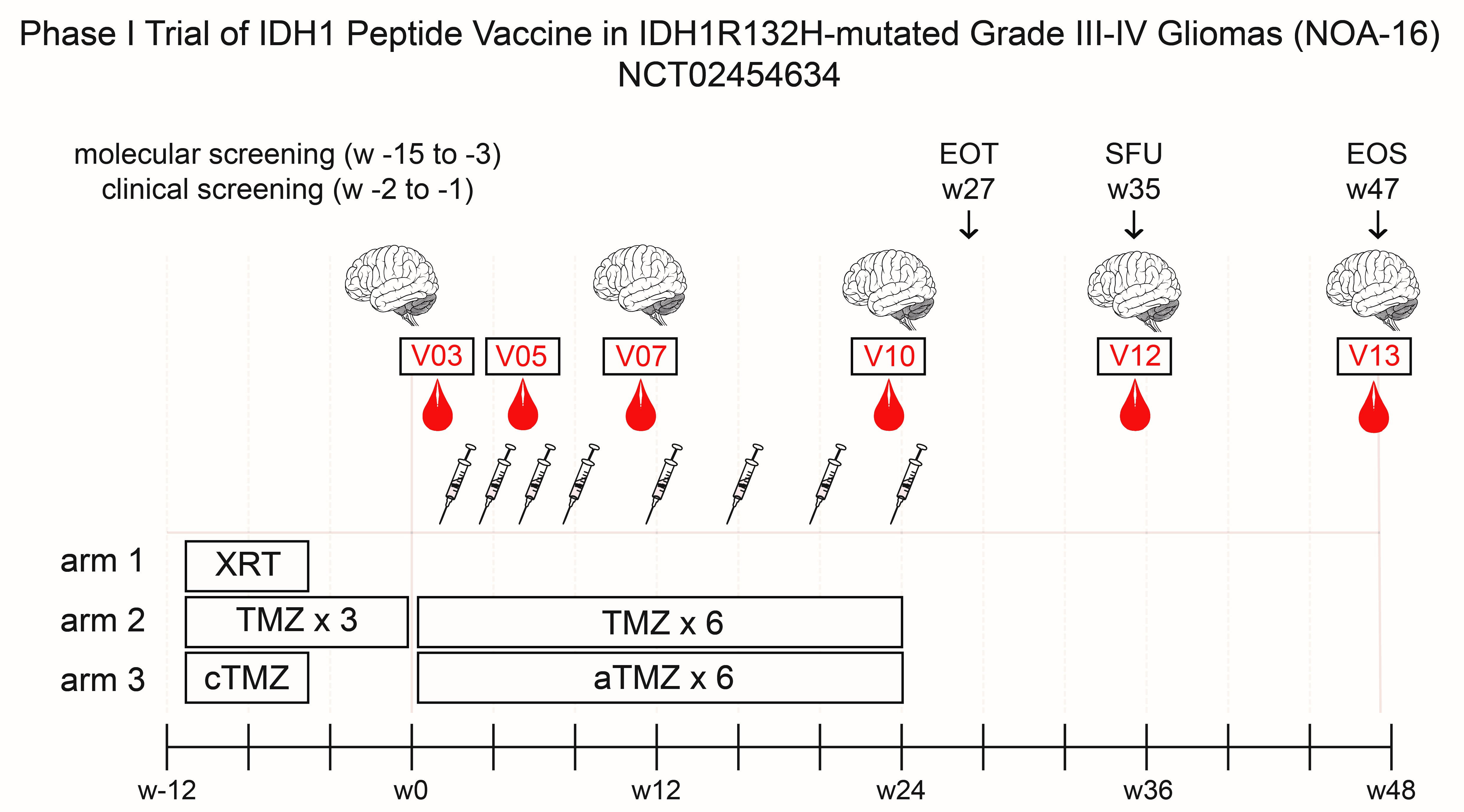

In the most recent edition of Nature, we are excited to report on the successful completion of our first-in-human phase I clinical trial (NOA16, NCT02454634) targeting a shared clonal driver mutation using a peptide vaccine in diffusely infiltrating low grade and anaplastic astrocytoma, a type of malignant brain tumor affecting remarkably young patients.
It was more than 10 years ago that – over a bottle of beer with a friend and collaborator – the idea to develop a peptide vaccine targeting the most common IDH mutation in glioma, IDH1R132H as a potential neoepitope, was conceived. We started the project in our lab at the German Cancer Research Center and the University Clinic Heidelberg – a junior research group at that time, when little was known about the biology of this just discovered mutation. After seeing the first results of mutation-specific immune responses, we were taken a little aback when we did not observe CD8+ T cell responses against IDH1R132H. At that time, there was little interest in CD4+ T helper cells as targets for neoepitope-specific antitumor immunity. We proceeded to explore mutation-specific T helper cell responses in a major histocompatibility complex (MHC)-humanized mouse model and developed a peptide vaccine capable of controlling IDH1-mutant tumors by inducing mutation-specific T helper cells and antibodies.
As a research group with a strong focus on clinical translation, we have been and still are embedded in an excellent institutional, infrastructural, and intellectual network on campus in Heidelberg, connecting the University Clinic Heidelberg (sponsor of the clinical study), the German Cancer Research Center, and the National Center for Tumor Diseases (NCT). The framework of the German Neurooncology Working Group (NOA) of the German Cancer Society, a network that is dedicated to jointly perform national clinical trials in neurooncology, enabled us to join forces with eight excellent neurooncology sites in Germany to initiate – and successfully complete – a first-in-human phase I German wide multicenter trial. Its primary endpoints, safety and immunogenicity, were both clearly met.
Yet, when conceptualizing the trial, we aimed for more: scientific understanding in order to develop this immunotherapeutic approach further, preclinically and clinically. Thus, we included comprehensive immune monitoring for this trial. Performing central immune monitoring at the NCT Heidelberg for a multicenter trial creates both chances and challenges. In preparation of the trial, sample handling, processing and shipping were strictly coordinated and harmonized, requiring complex logistics, while all analyses were performed centrally, allowing maximum standardization and consistency. Once having reached bedside, our scientific curiosity and mission to improve and optimize immunotherapeutic approaches, drove us to – and comprehensive sampling enabled us to – go back to bench and exploit datasets and sample sets to understand biological and cellular mechanisms of the vaccine and vaccine-induced T cells. We were able to confirm the importance and relevance of CD4+ T helper cells, which we had observed in our preclinical mouse models, in the clinical trial. By comprehensively integrating cellular immune monitoring, incl. T cell receptor sequencing and antigen specificity assays, clinical and survival as well as imaging data, we could show the following: The vaccine induced target-specific T cells that were CD4+ T helper cells of TH1 and TH17 types, while mutation-specific CD8+ T cells were lacking – just like in the MHC-humanized mouse model. Neither survival nor immune responses were associated with known molecular prognostic determinants. A remarkably high rate of pseudoprogression, a clear indicator of local inflammation that manifests as contrast enhancement in magnetic resonance imaging similar to a tumor, was associated with vaccine-induced immune responses. In the NOA16 cohort, we had the unique chance to freshly analyze such a post-vaccine tissue lesion that was at the time considered and later confirmed to be a pseudoprogression. This sample turned out to be the most precious sample of the study: We found massive T cell infiltration, with target antigen-specific T cells present. We performed single cell RNA and VDJ sequencing on these T cells to characterize transcriptomic landscapes and T cell receptors. In parallel, we had set up a bioinformatics platform and a pipeline for identifying TCR by single cell VDJ sequencing, integrating transcriptomic data, as well as cloning and testing identified TCR. Applying this workflow, we were thrilled to identify a target antigen-specific TCR on CD4+ T cells, and at the same time explore the transcriptomic signature of these clonal T cells within this pseudoprogressive lesion of the vaccinated patient.
These analyses allowed us a mechanistic glimpse on phenotype, functionality and anti-tumor efficacy of vaccine-induced T cells in the CNS, confirming and emphasizing the relevance of antigen-specific CD4+ T helper cells for cancer immunotherapy. Altogether, our journey from the idea over a bottle of beer to the successful completion of a multicenter phase I study, all in one hand, has broadened our understanding of anti-tumor immunity and antigen-specific T cells in the CNS. However, we have not yet reached our final destination. This is just a stopover on the road towards implementing specific immunotherapy targeting driver mutations in cancer. The advantageous nature of the antigen – shared, unique, clonal – encourages us to assess the efficacy of IDH1-vac in a placebo-controlled follow up phase 2 trial and explore novel approaches to optimize IDH1 mutant-specific immunotherapies.
Follow the Topic
-
Nature
A weekly international journal publishing the finest peer-reviewed research in all fields of science and technology on the basis of its originality, importance, interdisciplinary interest, timeliness, accessibility, elegance and surprising conclusions.

Related Collections
With Collections, you can get published faster and increase your visibility.
Carbon Dioxide Removal
Publishing Model: Hybrid
Deadline: Jan 16, 2027





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in