Understanding Contraceptive Intentions in Ethiopia: A Story of Barriers, Beliefs, and Empowerment
Published in Anatomy & Physiology
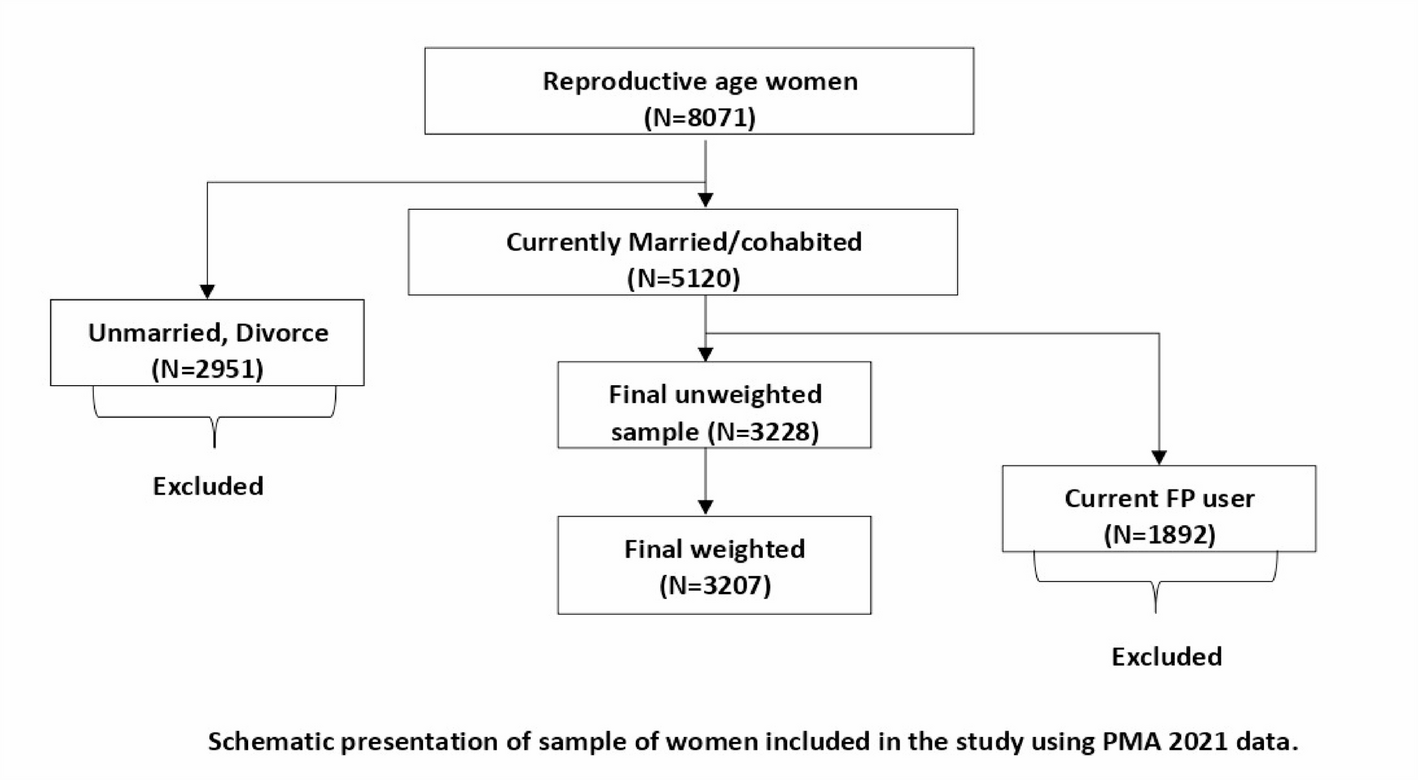
As a public health researcher in Ethiopia, I’ve witnessed firsthand how limited access to contraception impacts women’s lives—from health risks to economic and educational barriers. But beyond access, attitudes play a critical role. Myths about side effects, partner opposition, and religious beliefs often overshadow the benefits of family planning. This study aimed to move beyond statistics and understand the human stories behind non-use.
Key Findings: What Women Told Us
-
Attitudes Matter: Fear of side effects (real or perceived) was the most cited deterrent—even more than access.
-
The Power of Social Norms: Many women said their partners or communities viewed contraception as "unnatural," creating silent pressure to avoid it.
-
Agency vs. Obstacles: Women who felt confident in their ability to use contraceptives (self-efficacy) were more likely to intend to adopt them—but misinformation eroded this confidence.
Why This Matters
Policymakers often focus on increasing access to contraceptives (which remains vital), but our findings highlight the need for parallel interventions:-
Community dialogues to dispel myths.
-
Programs engaging men and religious leaders.
-
Counseling that addresses fears and builds self-efficacy.
A Personal Reflection
One interview stayed with me: a woman whispered that she secretly desired contraception but feared her husband would accuse her of "infidelity." Her story underscored how deeply gender dynamics intertwine with health choices. Research isn’t just about data, it’s about giving voice to these unspoken struggles.Join the Conversation
I invite you to read our full article [Contraceptive use intention and determinants among nonuser reproductive-aged married women in Ethiopia based on the theory of planned behavior | Discover Public Health] and reflect: -
Follow the Topic
-
Discover Public Health
This is an open access journal publishing research from all fields relevant to public health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Antimicrobial Resistance: The New Challenge to Global Health in a Post-Pandemic World
Antimicrobial resistance (AMR) is a seriously ongoing threat to global health, occurring when bacteria, fungi, viruses, and parasites evolve to resist the drugs designed to kill or block them. The COVID-19 pandemic has both directly and indirectly exacerbated the problem of AMR, as the overuse of antibiotics has accelerated the development of resistance in many pathogens. COVID-19 may have subsided, but AMR continues to pose a significant risk to the effectiveness of global healthcare systems, threatening to reverse decades of progress in combating infectious diseases. The interplay between population health and AMR has become increasingly critical as healthcare practices have shifted in response to the pandemic. Understanding this relationship is essential for developing effective strategies to mitigate the impact of AMR on population health in a post-COVID context.
The motivation for launching this Collection arises from the urgent need to address the rising tide of AMR as healthcare systems grapple with the long-term effects of the pandemic. Increased antibiotic use during COVID-19 treatment, changes in healthcare access, and disruptions in public health interventions have all contributed to an environment where AMR can thrive. Moreover, the pandemic has highlighted the importance of a multidisciplinary approach to tackling AMR, involving epidemiology, policymaking, and community health initiatives. This Collection aims to provide a platform for researchers and practitioners to share insights and findings that can inform future strategies to combat AMR while considering the broader implications for population health.
This Collection aims to highlight the multifaceted nature of AMR in a post-pandemic environment. We solicit articles that investigate the particular issues provided by the pandemic in terms of AMR development and containment, examine the impact of AMR on many sectors of healthcare, and propose novel strategies to minimize resistance propagation. Submissions may include original research, policy assessments, program evaluations, and comments on the following major areas:
• Epidemiology and trends of AMR post-pandemic
• Impact of COVID-19 on antibiotic usage
• Surveillance strategies for AMR
• AMR and stewardship
• Prevention and control measures to limit AMR spread
• Policies and programs to promote antibiotic stewardship
• Economic and social implications of AMR
• Global collaboration and initiatives to tackle AMR
By addressing these critical issues, this Collection aims to provide a comprehensive understanding of the emerging challenges in antimicrobial resistance in a post-pandemic world and to promote effective strategies to preserve the power of our current antimicrobials.
Keywords: antimicrobial resistance; COVID-19; antibiotics; global health; infectious diseases; public health; policy; prevention
This Collection supports and amplifies research related to SDG 3.
Publishing Model: Open Access
Deadline: Jun 30, 2026
Digital Frontiers in Public Health: Data-driven Solutions and Technologies for Efficiency, Effectiveness, and Equity
In recent years, the landscape of public health has been transformed by unprecedented access to high-quality data, advances in data storage and processing, and a growing willingness to share information across jurisdictions. The global response to the COVID-19 pandemic exemplified how coordinated data use and technological innovation can accelerate decision-making, enhance surveillance, and save lives. These developments mark a new era in which the application of modern data analytics in evidence-driven public health practices is not only possible but essential.
Building on this momentum, contemporary innovations are contributing to significant improvements in the three Es of public health: efficiency, effectiveness, and equity. Improved efficiency enables resources to be allocated and managed in a manner that generates the maximum attainable outputs; enhanced effectiveness ensures that public health policies, interventions, and practices achieve the expected health outcomes; and strengthened equity promotes fair access to healthcare and public health services across all populations. Together, these dimensions reflect the evolving priorities and capabilities of modern public health systems.
This Collection, “Digital Frontiers in Public Health: Data-driven Solutions and Technologies for Efficiency, Effectiveness, and Equity,” invites contributions that explore these themes through empirical studies, methodological advancements, case studies, and policy analyses. We seek manuscripts that highlight innovative data applications, cross-sector collaborations, digital health initiatives, and strategies that enhance equity through technology and data integration, as well as collaborative public health practices.
Topics of interest include, but are not limited to:
- Applications of novel data linkage and analytics methods in public health
- The role of participation and co-creation in addressing public health issues
- Digital and technological innovations in public health
- Complete or partial assessments of triple Es in public health
- Economic evaluations of public health interventions
By showcasing diverse approaches from around the world, this Collection aims to provide a comprehensive overview of how data-driven innovations are reshaping public health practice today, and in the future. Researchers, practitioners, and policymakers are encouraged to share their insights and experiences to contribute to this critical dialogue on the future of public health.
This Collection supports and amplifies research related to SDG 3.
Keywords: digital applications; data sharing; data infrastructure; economic evaluations; health equity; public health; policy analysis; health informatics
Publishing Model: Open Access
Deadline: Sep 30, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in