World Population Day 2026: Behind the Paper Interview with Mohamed Ismail
Published in Social Sciences, Mathematics, and Economics

Mohamed Ismail is Director of Analytical Research Ltd, and an Affiliate Research Fellow at the Oxford Institute of Population Ageing, University of Oxford. Trained in engineering, computer science, and mathematical finance, he began his career as a quantitative analyst in the City of London, working with major global financial institutions including Merrill Lynch, HSBC, Mizuho, and Credit Suisse. Since 2009, he has focused on quantitative social research, applying advanced statistical and mathematical modelling techniques to large and complex datasets. He collaborates internationally, has published in peer-reviewed journals, and regularly delivers invited talks.
His current research explores how mathematical and dynamical systems can inform our understanding of population ageing, particularly in relation to health and social care.
- How can countries prepare health systems for rapidly increasing long-term care needs driven by population ageing?
Most health systems were built to treat acute illness, things like a heart attack, an infection or a broken hip, and then send people home. Ageing populations need something the system was never really designed for: ongoing help with everyday tasks for people living with chronic conditions, disability and a gradual loss of function, often over many years. In many low- and middle-income countries, that shift is arriving faster than institutions can adapt to it.
The honest starting point is that most governments don’t know the scale of the problem they face. They can usually tell you how many older people live in the country, but not how many of them struggle to wash, dress, cook or move around without help. When that information is missing, planning becomes a reaction to crisis rather than something done in advance.
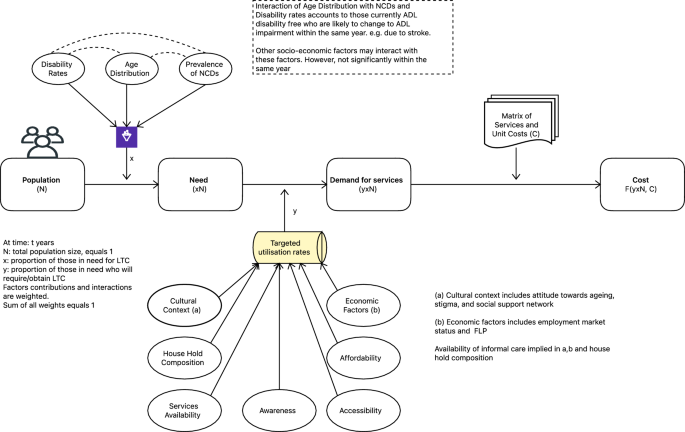
That gap is what our recent work tried to address. We built the LTC Needs Index to produce a population-level estimate of who is likely to need care, drawing on demographic and disease data that countries already collect rather than waiting for surveys that may be years away. An estimate is only a first step, though. The harder task is to start treating long-term care as part of mainstream health planning, including its financing, workforce and services, while there is still time to build it, rather than scrambling once the pressure has already arrived.
- What role do non-communicable diseases play in shaping future care dependency and health system demand?
Non-communicable diseases sit right at the centre of this. Diabetes, cardiovascular disease, dementia and Parkinson’s are usually discussed as causes of death, but they are also among the main routes by which people come to need daily care, because of the disability and functional decline that follow them.
In our study, recorded disability remained the strongest single driver of care need in seven of the eight countries we examined. What struck us was how much the diseases behind that need varied from one country to the next. Qatar was the exception: there, diabetes accounted for a larger share of estimated care need, close to 39 per cent, than disability did. That is a very different picture from Saudi Arabia, where disability on its own explains most of the need.
So, the practical conclusion, for me, is that you cannot really draw a clean line between chronic disease policy and long-term care policy; they are the same conversation. A country that manages diabetes and heart disease well, and picks up cognitive decline early, is also reducing the number of people who will need intensive care later. In that sense, money spent on prevention is already long-term care spending, and it simply shows up earlier in the system.
- Why is investing in data on ageing, disability, and care needs essential for achieving equitable health outcomes?
This is an equity question more than a technical one. The evidence shows that long-term care needs are not distributed evenly across a population; they are strongly tied to factors such as income, gender, disability and where people live. Yet across much of the world, particularly in lower-income regions, almost none of that is measured systematically.
The result is a real blind spot in policy. A government may have a good count of its older population while having no clear idea how many of those people need help with basic tasks such as eating or bathing, or with the more complex activities of daily living like managing money and medication. If you can’t see who is going without support, you can’t direct help to them, and resources tend to flow to wherever demand is loudest rather than to where the need is greatest.
Better data on ageing and disability lets policymakers identify unmet needs, share resources fairly and design services around how vulnerability is distributed rather than around assumptions. Without it, the people least able to advocate for themselves are usually the ones who stay invisible.
- How can integrating long-term care into universal health coverage strengthen SDG 3 in ageing societies?
Universal health coverage is usually framed around getting people access to treatment, but ageing well takes more than treatment. It takes sustained support with daily life, and that is exactly the part that tends to lie outside the package.
When long-term care is left out of universal coverage, a particular group slips through the middle: older adults living with disability or chronic illness whose needs are treated as too ‘social’ for the health system and too ‘medical’ for whatever social care exists. They end up belonging to neither. Bringing long-term care inside universal coverage closes that gap. It nudges systems towards earlier intervention, rehabilitation and steady support, rather than waiting for the fall, the stroke or the hospital admission that could often have been delayed or avoided. That matters more as people live longer, because living longer only counts for much if those extra years come with enough support to live them reasonably well.
- What strategies can reduce reliance on informal caregivers and promote more sustainable, inclusive care systems?
Take the MENA region as an example. There, long-term care is still carried almost entirely by families, and overwhelmingly by women. The WHO estimates that across much of MENA, somewhere between 80 and 95 per cent of it is provided by unpaid female relatives. That work is largely invisible, and it carries real costs to women’s health, to their earnings, and to their ability to stay in paid employment. Easing that burden means building the alternatives that barely exist in many countries: home care and community services, rehabilitation, and a trained, paid care workforce. It also means supporting the family carers who will remain central for a long time yet, through respite, training and some form of financial protection, instead of simply taking their labour for granted. One thing our results kept showing is that there is no single template for this. The balance between disability and disease, and therefore the kind of care a country needs, looks quite different in Morocco than it does in Qatar. What holds everywhere is the timing: it is far easier to build these systems incrementally, ahead of the demographic shift, than to assemble them in a hurry once that shift has already happened.
Thank you for joining and sharing, Dr Ismail!
#WorldPopulationDay #WorldPopulationDay2026 #PopulationMatters #GlobalAwareness #SustainableDevelopment #July11
Follow the Topic
-
Population Health Metrics
Population Health Metrics aims to advance the science of population health assessment, and welcomes papers relating to concepts, methods, ethics, applications, and summary measures of population health.

Related Collections
With Collections, you can get published faster and increase your visibility.
Open Issues in Population Health Modeling: Methodological, and Epidemiological Implications of Continuous Changes in Population Dynamics
Among the Sustainable Development Goals (SDGs), SDG 3 focuses on ensuring healthy lives and promoting well-being for people of all ages, combating communicable diseases, lowering mortality rates from non-communicable diseases, and promoting mental health. Indeed, a sustainable society fundamentally depends on the number of years its members can actively contribute to social and economic activities, which requires living in good health. Therefore, the concepts of lifespan, longevity, and health are intrinsically crucial when evaluating and planning sustainability policies for both the short and long term.
In this context, socio-political decision-makers can greatly benefit from long-term estimates derived from methodological advancements in the demographic and health domains. Such advancements can fuel new perspectives and theories within their respective fields. The development and application of rigorous quantitative methods not only refine data interpretation but also foster a deeper understanding of underlying social, health, and population dynamics. These innovations enable researchers to challenge existing paradigms, paving the way for more robust theoretical developments in public health and population studies.
This Collection seeks cutting-edge articles that advance theories and evidence related to longevity and population health metrics. We particularly encourage research focused on elegant methods for measuring health dynamics and forecasting changes in longevity around the globe. Contributions that advance the state of the art in the field, while embracing rigorous methodological approaches, are highly welcomed.
This Collection supports and amplifies research related to SDG 3, Good Health and Well-Being.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Jul 30, 2026
Advancing the Measurement of Social Connection for Population Health: New Evidence, Metrics, and Global Priorities
Social connection is increasingly recognized as a vital component of population health. It includes the structure of social networks, the support that flows through relationships, and the quality of interactions that contribute to well-being. Research across multiple disciplines has established that limited or poor social connection is linked to higher risks of premature mortality, mental health problems, cardiovascular disease, cognitive decline, lower educational attainment, and reduced economic participation. These findings highlight the need for rigorous and comparable metrics that can illuminate the distribution, determinants, and consequences of social disconnection at scale.
Despite a growing interest in social connection, population level measurement remains uneven. Studies often rely on single items, short scales, or constructs that capture only one aspect of the broader social landscape. Loneliness, social isolation, and social support are frequently treated as interchangeable, even though each reflects a different dimension of social life and may influence health through distinct pathways. In many settings, there is no routine surveillance of social connection. As a result, policymakers and practitioners lack the data needed to design effective interventions or monitor changes over time.
Conceptual clarity is a prerequisite for measurement. Social connection is multidimensional and includes the size and diversity of social networks, the availability of emotional or instrumental support, and the positive or negative qualities of relationships. Social isolation is the objective absence of social roles or interactions. Loneliness is the subjective experience of wanting more or better connection than one currently has. These concepts intersect but are not synonymous. Accurate assessment requires tools that reflect each dimension and that can be adapted or validated across cultures, languages, and life stages.
Research from low and middle income countries is particularly limited even though many of these settings experience social conditions that may heighten vulnerability to social disconnection. Large and rapid demographic transitions, urban migration, changing family structures, economic insecurity, and exposure to conflict or displacement can all shape patterns of social connection. Yet most validated instruments originate in high income countries, and many have not been adapted or tested for linguistic, cultural, and contextual relevance in LMIC populations.
The need for strong metrics extends beyond conceptual work. The use of digital technology, demographic change, shifting household structures, migration, and urbanization all influence how social connections form and function. These forces create new opportunities for measurement, such as digital interaction data or innovative mixed-method approaches, but they also introduce new challenges. Measures grounded in one cultural or linguistic context may not translate easily to another. Children, adolescents, older adults, and marginalized groups may require tailored instruments that reflect their social realities. Community and policy interventions also need evaluation frameworks that capture both intended and unintended effects on connection.
This special issue invites research that advances the science of measuring social connection for population health. Relevant contributions include but are not limited to:
1. New conceptual models and frameworks for assessing social connection at scale
2. Validation or adaptation of measurement instruments across cultures and population groups
3. Methods for distinguishing between loneliness, social isolation, and social support in surveillance systems
4. Epidemiologic analyses that examine levels, patterns, and trends in social connection
5. Studies linking social connection metrics with health, economic, or educational outcomes
6. Approaches to integrating social connection into existing population health surveys
7. Measurement of social connection in digital and hybrid social environments
8. Evaluation metrics for policies, community initiatives, and individual level interventions
9. Proposals for harmonized indicators that support international comparisons
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Aug 28, 2026





Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in