Singapore Government Co-funding and Subsidies for Private IVF Treatment - A Policy Risk Assessment White Paper
Published in Social Sciences, General & Internal Medicine, and Pharmacy & Pharmacology
Please refer to the following news media articles:
Singapore should beware of the pitfalls of subsidizing private IVF treatment
Issues to consider in co-funding private IVF treatment
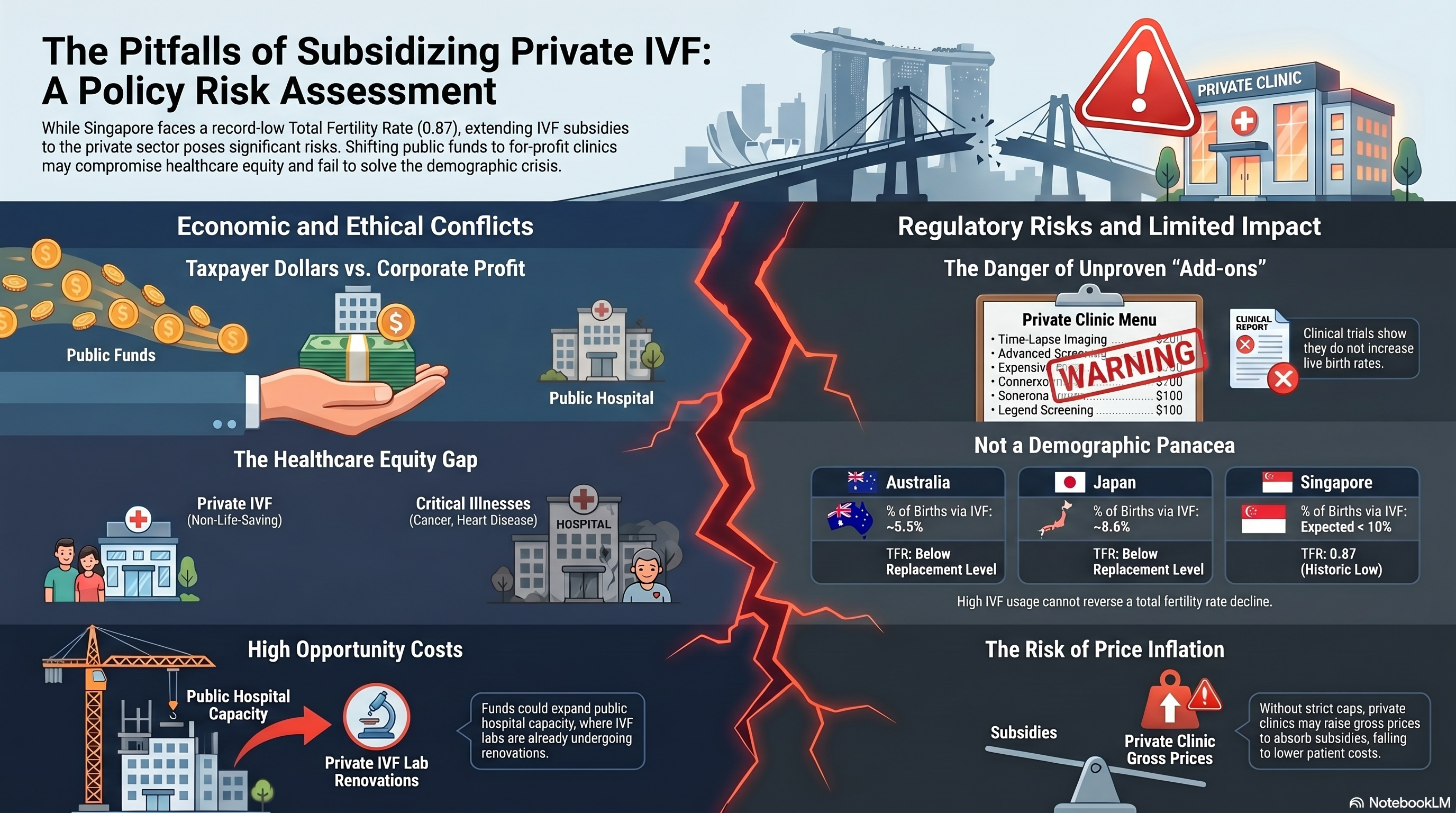
Summary: Singapore faces a severe demographic crisis, with its total fertility rate (TFR) falling to a historic low of 0.87 births per woman in 2025. In response to this existential challenge, policymakers have debated extending government co-funding for in vitro fertilization (IVF) to private fertility clinics. Proponents argue that such a move would alleviate long waiting times at public hospitals, which currently enjoy exclusive subsidies, thereby mitigating the age-related decline in female fertility and improving overall IVF success rates. However, this paper critically evaluates the potential pitfalls of subsidizing private IVF treatment. Key concerns include the diversion of public funds to maximize shareholder profits rather than enhancing public healthcare infrastructure, and the inequity of prioritizing non-life-saving fertility treatments over critical illnesses within the private sector. Furthermore, the paper highlights the necessity of stringent regulations, such as mandating equivalent or superior success rates, controlling gross prices, and preventing the exploitation of vulnerable patients through unproven add-on procedures. Ultimately, while extending subsidies may serve as a symbolic gesture of support for childless couples, its actual demographic impact is likely marginal, necessitating a prudent assessment of healthcare resource allocation and opportunity costs.
Keywords: Total Fertility Rate; In Vitro Fertilization; Healthcare Subsidies; Private Healthcare; Pronatalist Policy; Singapore Demographics
1. Introduction
Singapore is currently confronting a profound demographic crisis. In 2025, the nation's total fertility rate (TFR) plummeted to an unprecedented historic low of 0.87 births per woman, a significant drop from the previous record lows of 0.97 recorded in both 2023 and 2024 [1]. Deputy Prime Minister Gan Kim Yong warned in Parliament that if no new measures are taken, Singapore's citizen population will start to shrink by the early 2040s, with every 100 residents today producing only 44 children and 19 grandchildren [1]. This persistent decline has generated considerable consternation among government policymakers, who perceive the demographic crunch as an existential threat to Singapore's future economic growth, societal stability, and national survival. The International Monetary Fund has noted that Singapore's experience in trying to raise its fertility rate offers cautionary lessons for other countries, emphasizing that access to IVF and other reproductive technologies alone is not sufficient to ensure that older women have enough babies to compensate for fertility decline among younger women [2].
As part of its comprehensive pronatalist strategy, the Singaporean government currently offers substantial financial support to couples seeking assisted reproductive technology (ART). Eligible women under the age of 40 can receive up to 75% in government co-funding for up to three fresh and three frozen IVF cycles, provided the treatment is undertaken at public assisted reproduction (AR) centres [3] [4]. Women over 40 are also eligible for co-funding for up to two cycles, contingent upon having attempted at least one IVF or intrauterine insemination (IUI) cycle before reaching the age of 40 [4]. However, a significant challenge within this subsidized framework is the heavy patient load at public hospitals, which has led to prolonged waiting times for treatment [5]. In 2023, the Ministry of Health reported that median and mean wait times across public hospitals were no more than seven and twelve days, respectively, for the first assisted reproductive treatment appointment [5]; however, the broader treatment journey—from initial consultation to commencing an IVF cycle—can extend considerably longer, particularly for subsidized patients [6].
Because female fertility, particularly oocyte quality and quantity, declines sharply with age—especially after the mid-30s—there are profound concerns that extended waits at public clinics may detrimentally impact the IVF success rates of older patients [7] [8]. Consequently, there have been growing calls to extend government IVF subsidies to the private healthcare sector [9]. Proponents argue that this extension would alleviate the bottleneck at public hospitals, enabling patients to access high-quality medical care more swiftly and thereby boosting their chances of a successful pregnancy [9]. Despite these potential benefits, such a policy shift entails significant pitfalls and complex ethical, economic, and regulatory considerations that the Singapore government must carefully navigate.
2. The Economic and Ethical Dilemmas of Subsidizing Private IVF
2.1 Profit Maximization Versus Public Benefit
A fundamental distinction between public and private healthcare entities lies in their core objectives and accountability structures. Public hospitals are accountable to the government and the citizenry, prioritizing public health outcomes and equitable access to care [10]. Conversely, private healthcare institutions operate on a for-profit model, beholden to shareholders to maximize financial returns [11]. Research on private equity involvement in reproductive medicine has underscored that profit-driven incentives can influence clinical decision-making, potentially leading to the performance of more expensive, riskier, or scientifically unproven procedures [11]. If public funds were utilized to subsidize IVF treatments in private clinics, a substantial portion of taxpayers' money would invariably translate into corporate profits and shareholder dividends, rather than being reinvested into the national healthcare infrastructure [9].
This dynamic raises a critical question regarding the opportunity cost of resource allocation. Rather than channeling public funds into the private sector, the same financial resources could be utilized to expand and upgrade IVF facilities within public hospitals [9]. Investments could be directed toward hiring additional fertility specialists, expanding laboratory capacities, and acquiring advanced equipment, thereby directly reducing waiting times while retaining the funds within the public domain for the broader benefit of the population. The Singapore Ministry of Health's own parliamentary response in 2023 acknowledged that public AR centres were already expanding—with the National University Hospital completing renovations of its IVF laboratory in 2022 and KK Women's and Children's Hospital building a second IVF laboratory—suggesting that capacity expansion within the public sector is a viable and ongoing alternative [6].
2.2 Healthcare Equity and Resource Allocation
The proposal to subsidize private IVF treatments also introduces profound questions regarding fairness and equity in healthcare financing [12]. In publicly funded healthcare systems, the allocation of limited resources is a pressing ethical issue, as expenditure on one disease or intervention necessarily precludes spending on another [12]. Infertility, while deeply distressing and psychologically impactful, is generally not classified as a life-threatening or debilitating medical condition in the same category as cancer, stroke, or cardiovascular and renal diseases [13]. If the government sets a precedent by subsidizing IVF in private clinics, it invites legitimate scrutiny regarding the absence of similar subsidies for the private treatment of these severe, life-threatening conditions [9].
From a public health ethics perspective, prioritizing public funding for non-life-saving fertility treatments in the private sector over critical illnesses represents a potential misallocation of resources [12]. The Ministry of Health bears a moral imperative and public duty to ensure that taxpayers' money is spent prudently to address the most urgent and impactful healthcare needs of the population [9]. While infertility treatment has been argued to generate value beyond conventional quality-adjusted life year (QALY) metrics—given that it creates new lives—this argument does not straightforwardly resolve the equity concerns that arise when such treatment is prioritized in the private sector over life-saving interventions [13].
3. Regulatory Prerequisites for Private Subsidies
Should the Singapore government proceed with extending co-funding to private IVF clinics, stringent regulatory frameworks must be established to safeguard public funds and protect vulnerable patients. The Ministry of Health's 2023 parliamentary response indicated that any review of extending co-funding would need to assess how best to ensure clinical outcomes are monitored and acceptable, that couples are charged reasonably, and that co-funding monies are used prudently [6].
3.1 Mandating Success Rates and Independent Audits
To justify the expenditure of public coffers, any subsidy extended to a private IVF clinic must be contingent upon the clinic demonstrating IVF success rates that are equal to or higher than those achieved by public AR centres [9]. This requirement necessitates the implementation of rigorous, independent annual audits of private clinics' track records [9]. Linking subsidies to acceptable success rates serves a dual purpose. Firstly, it ensures value for money for the government and the taxpayer. Secondly, it acts as a deterrent against the exploitation of desperate patients who have very low prognoses for IVF success [9].
For instance, patients with severely diminished ovarian reserve—due to premature menopause or cancer chemotherapy—face significantly reduced chances of live birth through conventional IVF [14]. Similarly, patients with severe male-factor infertility requiring surgical extraction of immature sperm from the testes (testicular sperm extraction, TESE) face substantially lower success rates compared to patients with non-male-factor infertility [15]. By enforcing success rate benchmarks, private clinics would be incentivized to counsel such patients realistically, potentially directing them toward more viable alternatives such as oocyte or sperm donation, or adoption, rather than subjecting them to futile and emotionally draining treatment cycles [9]. The age-related decline in female fertility is well established: live birth rates per IVF cycle are approximately 42% for women under 35 years, declining to approximately 25% for women aged 38–40, and falling to less than 5% for women over 43 using their own eggs [7] [8].
3.2 Price Controls and Value for Money
Another critical regulatory measure is the stringent control of the gross price of IVF treatments before subsidies are applied [9]. Without robust price regulation, the introduction of government co-funding could inadvertently serve as a catalyst for private clinics to inflate their medical fees, thereby absorbing the subsidy to maximize profitability without reducing the out-of-pocket financial burden on the patient [9]. Ensuring "value for money" for both patients and the government requires transparent pricing structures, mandatory fee disclosure, and enforceable caps to prevent opportunistic price escalation.
3.3 Mitigating the Risk of Unproven Add-On Procedures
The influx of subsidized funding may leave patients with additional disposable income for medical fees, creating an environment in which practitioners might encourage uptake of costly ancillary IVF "add-on" procedures with dubious therapeutic value [9] [16]. Regulatory bodies such as the UK's Human Fertilisation and Embryology Authority (HFEA) have established evidence-based "traffic light" rating systems to evaluate the clinical evidence base for these adjunct treatments, providing a model that Singapore could adapt [17].
Many popular add-ons lack robust clinical evidence supporting their efficacy in improving live birth rates [16] [17]. A prominent example is the use of time-lapse imaging (TLI) systems for embryo incubation and selection, which relies on morphokinetic algorithms and artificial intelligence to purportedly identify the most viable embryos [18]. However, the landmark TILT trial—a multicentre, three-parallel-group, double-blind, randomized controlled trial published in The Lancet in 2024—demonstrated conclusively that TLI does not significantly increase the odds of live birth compared to standard care without time-lapse imaging (live birth rates: 33.7% in the TLI group versus 33.0% in the standard care group; adjusted odds ratio 1.04, 97.5% CI 0.73 to 1.47) [19]. Consequently, the HFEA does not recommend the routine use of TLI for improving IVF success rates [17].
Other procedures have received even more cautionary assessments. Preimplantation genetic testing for aneuploidy (PGT-A) has been widely adopted despite lacking a complete evidence base, with some studies suggesting that it may not improve—and could potentially reduce—live birth rates in certain patient populations [20]. Endometrial receptivity testing (ERA) aims to individualize embryo transfer timing, but systematic reviews have found insufficient evidence to support its routine clinical use [21]. Various immunological tests and treatments, including intralipids, intravenous immunoglobulin (IVIG), and glucocorticoids, have similarly been flagged by the HFEA as having limited or no evidence of benefit [17]. Stringent oversight is essential to prevent the commercial exploitation of these unproven technologies in a subsidized private setting.
4. The Demographic Impact of IVF Subsidies: A Realistic Assessment
When evaluating the cost-benefit rationalization of extending IVF subsidies to the private sector, it is crucial to assess the realistic capacity of ART to reverse Singapore's macro-demographic decline. Statistical data from other advanced economies with well-developed IVF infrastructures provide instructive comparisons. In Australia, approximately 1 in 18 babies (roughly 5.5%) are conceived via IVF, representing one of the highest rates of ART utilization globally [22]. In Japan—which has the world's highest absolute number of IVF cycles performed annually—approximately 1 in 11.6 births (approximately 8.6%) are attributed to IVF [23]. Despite this, Japan continues to record one of the lowest fertility rates in the world, with its TFR remaining well below the replacement level of 2.1 births per woman [2].
Extrapolating these figures, even under optimal conditions, IVF is unlikely to boost the total number of births by more than 10% [9]. Given Singapore's extraordinarily low TFR of 0.87, a 10% increase in births via ART would barely move the needle toward the population replacement level. This observation aligns with the IMF's assessment that reproductive technologies are not a demographic panacea, and that Singapore's experience demonstrates that access to IVF is insufficient to compensate for fertility decline among younger women [2]. Pronatalist policies in Singapore, including the Baby Bonus scheme, childcare subsidies, and parental leave enhancements, have been studied extensively; research suggests that while financial incentives and work-life policies are perceived as supportive of childbearing, their overall effect on the TFR has been modest [24].
While extending co-funding to private clinics may serve a symbolic purpose—demonstrating the government's empathy and tangible support for childless couples navigating the arduous journey of assisted reproduction—the opportunity cost must be weighed carefully [9]. Critics argue that the substantial funds required for private IVF subsidies might yield a broader societal impact if reallocated toward enhancing childcare facilities, expanding preschool education subsidies, or improving work-life balance policies [9] [24]. Such broad-based family support measures are likely to benefit a vastly larger segment of the parenting population and may be more effective in encouraging couples to have multiple children.
5. Conclusion
Singapore's plummeting fertility rate necessitates decisive and multifaceted policy interventions. The proposal to extend government IVF co-funding to private fertility clinics aims to reduce waiting times and improve outcomes for older women facing age-related fertility decline. However, this approach is fraught with significant pitfalls. The diversion of public funds to profit-driven entities, the ethical dilemmas of prioritizing non-life-saving treatments over critical illnesses in the private sector, and the risk of exploiting vulnerable patients through unproven add-on procedures all demand rigorous scrutiny and careful policy design.
If the government pursues this policy, it must be accompanied by strict regulatory safeguards, including mandated and audited success rates, gross price controls, and stringent oversight of ancillary treatments. Ultimately, policymakers must recognize that while ART is a vital medical service for infertile couples, it is not a demographic panacea. The key question that Singapore must answer is how much value its citizens are receiving in return for the expenditure of their tax dollars on subsidizing private IVF treatment. A holistic and prudent approach to public healthcare expenditure is essential to ensure that taxpayers' money is utilized equitably and effectively to address Singapore's complex and pressing societal needs.
6. References
- Ang HM. Singapore's fertility rate drops to historic low of 0.87 as country faces 'existential challenge': DPM Gan. Channel News Asia. 2026 Feb 26. Available from: https://www.channelnewsasia.com/singapore/total-fertility-rate-tfr-2025-record-low-citizen-population-5954306
- Tan PL. Reversing Demographic Decline: Lessons from Singapore on Raising Fertility Rates. Finance & Development, International Monetary Fund. 2020 Mar;57(1). Available from: https://www.imf.org/en/publications/fandd/issues/2020/03/lessons-from-singapore-on-raising-fertility-rates-tan
- Ministry of Health Singapore. Marriage and Parenthood Schemes: Co-funding for Assisted Conception Procedures. Available from: https://www.moh.gov.sg/managing-expenses/schemes-and-subsidies/marriage-and-parenthood-schemes/
- Made For Families Singapore. Co-Funding for Assisted Conception Procedures. 2026 Mar 16. Available from: https://www.madeforfamilies.gov.sg/support-measures/baby-prep/co-funding-for-assisted-conception-procedures
- Ministry of Health Singapore. Waiting time for first assisted reproductive treatment appointment at public hospitals in past five years. Parliamentary QA. 2024 Apr 3. Available from: https://www.moh.gov.sg/newsroom/waiting-time-for-first-assisted-reproductive-treatment-appointment-at-public-hospitals-in-past-five-years/
- Ministry of Health Singapore. Extension of Co-Funding for the Assisted Conception Procedures Scheme to Private Clinics. Parliamentary QA. 2023 Mar 20. Available from: https://www.moh.gov.sg/newsroom/extension-of-co-funding-for-the-assisted-conception-procedures-scheme-to-private-clinics/
- Templeton A, Morris JK, Parslow W. Factors that affect outcome of in-vitro fertilisation treatment. The Lancet. 1996;348(9039):1402-1406.
- Ubaldi FM, Cimadomo D, Vaiarelli A, Fabozzi G, Venturella R, Maggiulli R, Mazzilli R, Ferrero S, Rienzi L. Advanced Maternal Age in IVF: Still a Challenge? The Present and the Future of Its Treatment. Frontiers in Endocrinology. 2019;10:94.
- Kwan WT. Singapore should beware of the pitfalls of subsidizing private IVF treatment. BioEdge. Available from: https://bioedge.org/beginning-of-life-issues/ivf/singapore-should-beware-of-the-pitfalls-of-subsidizing-private-ivf-treatment/; and Kwan WT. Issues to consider in co-funding private IVF treatment. The Straits Times Forum. Available from: https://www.straitstimes.com/opinion/forum/forum-issues-to-consider-in-co-funding-private-ivf-treatment
- Daniels N. Resource Allocation and Priority Setting. In: Barrett DH, Ortiz LW, Dawson AL, Saenz C, Reis A, Bolan G, editors. Public Health Ethics: Cases Spanning the Globe. Cham: Springer; 2016. p. 61-100.
- Zadeh AA, Bakkensen JB, Pal L, Seli E. Private equity and reproductive medicine: "Fertile breeding ground"–a physician's perspective. Reproductive Biology and Endocrinology. 2025;23(1):1-9.
- Seixas BV, Dionne F, Mitton C. Describing practices of priority setting and resource allocation in publicly funded health care systems of high-income countries. BMC Health Services Research. 2021;21(1):1-14.
- Keller E, Chambers GM, Ledger W, Boivin J, Bhattacharya S. Valuing infertility treatment: Why QALYs are inadequate, and an alternative approach to cost-effectiveness thresholds. Frontiers in Medical Technology. 2022;4:1053719.
- Navot D, Bergh RA, Williams MA, Garrisi GJ, Guzman I, Sandler B, Grunfeld L. Poor oocyte quality rather than implantation failure as a cause of age-related decline in female fertility. The Lancet. 1991;337(8755):1375-1377.
- Esteves SC, Roque M, Bradley CK, Garrido N. Reproductive outcomes of testicular versus ejaculated sperm for intracytoplasmic sperm injection among men with high levels of sperm DNA fragmentation in semen: systematic review and meta-analysis. Fertility and Sterility. 2017;108(3):456-467.
- Perrotta M, Boivin J, Jones C, Hammarberg K, Hamberger L, Tarlatzis B, Bhattacharya S. Exploring Fertility Treatment Add-On Transparency in the UK. Remaking Fertility. 2024. Available from: https://www.qmul.ac.uk/remakingfertility/media/remaking-fertility/Perrotta-et-al.,-2024.pdf
- Human Fertilisation and Embryology Authority. Treatment add-ons with limited evidence. 2023 Oct 16. Available from: https://www.hfea.gov.uk/treatments/treatment-add-ons/
- Mrugacz G, Grusza M, Lukaszuk K, Mrugacz M. Time-Lapse Imaging in IVF: Bridging the Gap Between Promises and Evidence. International Journal of Molecular Sciences. 2025;26(19):9609.
- Bhide P, Chan DYL, Lanz D, Alqawasmeh O, Barry E, Baxter D, Gonzalez Carreras F, Choudhury Y, Cheong Y, Chung JPW, Collins B, Cong L, Doidge S, Heighway J, Patel D, Pardo MC, Rattos A, Wright A, Dodds J, Perez T, Khan KS, Thangaratinam S. Clinical effectiveness and safety of time-lapse imaging systems for embryo incubation and selection in in-vitro fertilisation treatment (TILT): a multicentre, three-parallel-group, double-blind, randomised controlled trial. The Lancet. 2024;404(10449):256-265.
- Lensen S, Bhattacharya S, Wilkinson J. Evaluating the evidence for preimplantation genetic testing for aneuploidy. Fertility and Sterility. 2025.
- Clain E, Bhattacharya S, Maheshwari A. Endometrial receptivity, to test or not to test: the evidence. Best Practice & Research Clinical Obstetrics & Gynaecology. 2023;86:102302.
- Chalmers I, Glasziou P. One in 18 babies born in Australia are conceived via IVF. The Guardian. 2023 Sep 22. Available from: https://www.theguardian.com/australia-news/2023/sep/22/babies-born-via-ivf-australia-how-many-stats-data
- com. IVF Births in Japan Reach a Record 70,000 in 2021. 2023. Available from: https://www.nippon.com/en/japan-data/h01780/
- Tan J. Perceptions towards pronatalist policies in Singapore. Journal of Population Research. 2023;40(14).
Follow the Topic
Introducing: Social Science Matters
Social Science Matters is a campaign from the team at Palgrave Macmillan that aims to increase the visibility and impact of the social sciences
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in