Behind the Paper: Are IBS Medications as Safe as We Think?

If we are treating IBS with lifelong medications, how safe are these therapies over the long run?
Why we asked this question?
In clinical practice, IBS treatment is often a balancing act. There are several FDA approved medications specifically designed for IBS, alongside a wide range of other drugs used off label, especially antidepressants.
Antidepressants are commonly prescribed in IBS not just for mood, but for their presumed effects on the gut-brain axis. Many clinicians and patients assume they are safe when used long term. But surprisingly, there has been very little large scale data evaluating their safety over many years.
At the same time, newer IBS medications, those approved by regulatory agencies, are typically studied in clinical trials lasting months, not decades.
So we wondered
what happens when we look at real world patients over many years? Do these medications remain safe?
What we did
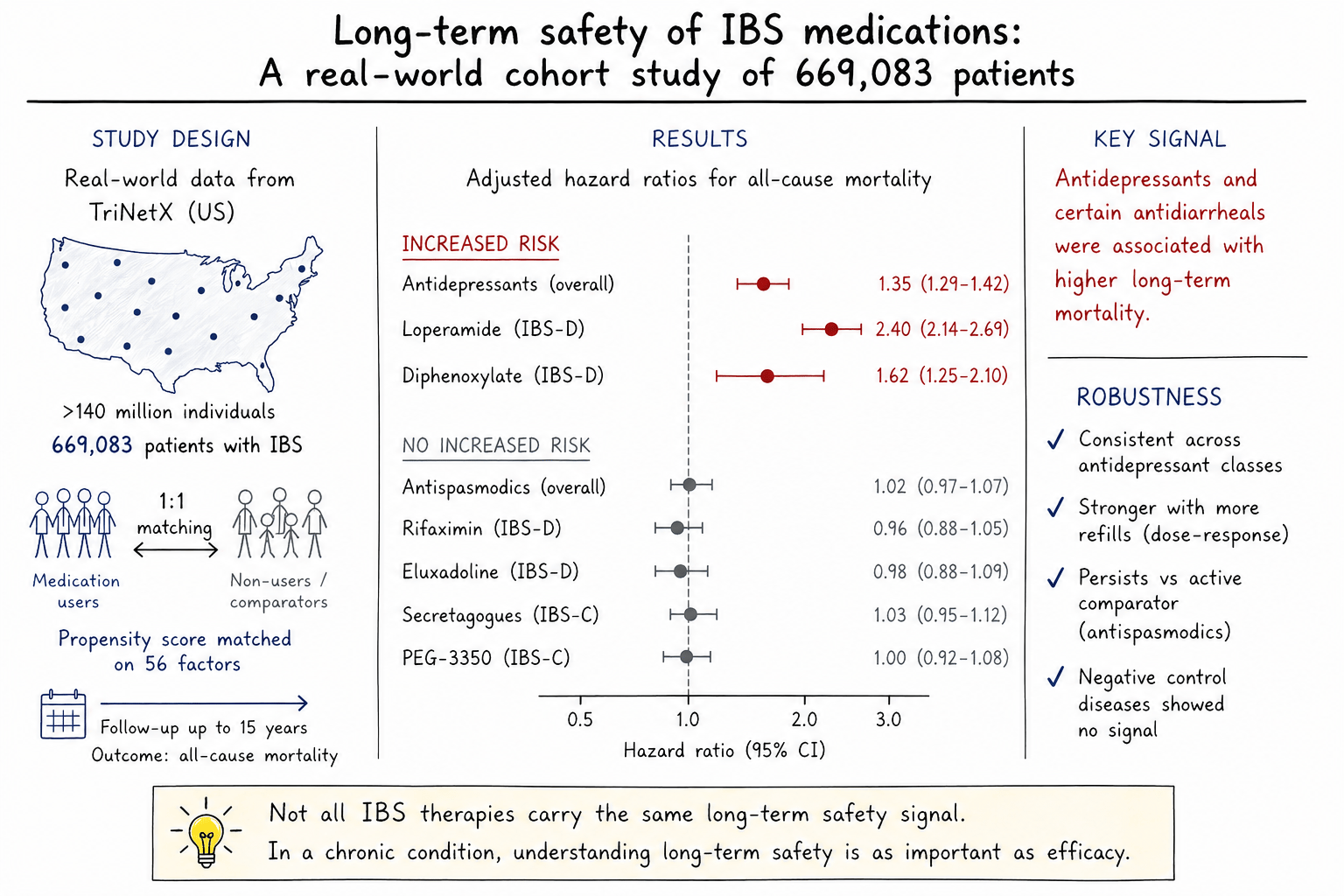
To answer this, we turned to a large nationwide United States electronic health record database, analyzing nearly 700,000 patients with IBS.
We designed the study carefully to mimic what a randomized clinical trial might look like in the real world. This approach, called target trial emulation, allowed us to compare patients who received specific medications with similar patients who did not.
To ensure fairness, we matched patients one to one based on 56 different characteristics, including age, sex, comorbidities, and other medications. This process, called propensity score matching, helps reduce bias and makes the comparison more reliable.
We then followed patients over time, sometimes for years, to see whether different medications were associated with differences in all-cause mortality.
What we found the reassuring part
Many commonly used IBS medications, especially those that are FDA approved, did not show an increased risk of death.
These include medications for constipation such as secretagogues and polyethylene glycol-3350 as well as medications for diarrhea such as rifaximin and bile acid sequestrants, antispasmodics such as dicyclomine and hyoscyamine.
These are medications that patients often take chronically, and our findings suggest that, at least in terms of mortality, they appear safe over the long term.
In a field where long-term data is often lacking, this provides a degree of reassurance for both clinicians and patients.
The unexpected signal
Antidepressants were consistently associated with an increased risk of mortality.
This was not a small or isolated effect. The association appeared across all subclasses including SSRIs, SNRIs, TCAs, and mirtazapine. This finding consistent across age, sex, BMI, and racial groups and become stronger with more refills, suggesting a dose or duration related pattern
Even when we compared antidepressants to an active alternative treatment such as antispasmodics, the signal remained.
We also observed that certain antidiarrheal medications, specifically mu receptor agonists like loperamide and diphenoxylate, were associated with increased mortality in patients with IBS- diarrhea subtype.
Could this make biological sense?
Whenever we see an unexpected association, the next question is: Is this real or just a statistical artifact?
One reason we believe this signal deserves attention is that it is biologically plausible.
Antidepressants are known to affect multiple systems in the body. Prior research has linked them to:
- Cardiac arrhythmias through QT prolongation
- Blood pressure changes
- Increased risk of falls
- Gastrointestinal (GI) bleeding
- Suicidal ideation
- Weight gain and metabolic changes
In our study, we also saw higher rates of conditions such as
- Heart disease including heart failure and arrhythmias
- Stroke
- Falls
- Aspiration pneumonia
- GI bleeding
- hypertension
- Suicidal ideation
These are pathways that plausibly contribute to increased mortality over time.
Similarly, medications like loperamide, when used excessively, are known to affect cardiac ion channels and can lead to dangerous arrhythmias.
So where does this leave us?
First, this is not a call to completely stop prescribing antidepressants in IBS. These medications can be effective for symptom control, and for some patients, the benefits can outweigh the risks.
However, our findings suggest that
We should be more thoughtful about long term use
We should regularly reassess whether the medication is still needed
We should consider alternative therapies, especially when effective options exist
It also raises an interesting clinical question
Are antidepressants helping IBS primarily through their central brain effects, or through other properties such as antihistamine or anticholinergic effects?
If the latter is true, it opens the door to more targeted therapies with potentially fewer systemic risks.
Perhaps the most important takeaway is this:
Not all IBS medications are equal when it comes to long term safety.
For years, treatment decisions in IBS have focused mainly on symptom relief. But as patients remain on these medications for longer periods, safety becomes just as important as efficacy.
Our study adds a new layer to that conversation.
What comes next?
Our findings need to be assessed in other population-based datasets capable to following patients long-term. Cause-specific mortality and the underlying mechanisms warrant further investigation. Future societal guidelines for the management of IBS should incorporate considerations of long-term safety across recommended treatment modalities. More importantly, greater emphasis should be placed on identifying the underlying causes of IBS and implementing targeted, mechanism-based therapies rather than relying on empiric treatment approaches.
Final thoughts
IBS is a chronic condition, and for many patients, treatment is a long-term journey.
As clinicians and researchers, we often focus on what works. But we must also ask what is safe, especially over years, not months?
This study is one step toward answering that question.
And perhaps most importantly, it reminds us that even familiar medications deserve to be re-examined with fresh eyes.
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Exercise and Physical Activity in Health and Disease
Publishing Model: Open Access
Deadline: Sep 03, 2026
Life Course Epidemiology
Publishing Model: Open Access
Deadline: Sep 30, 2026

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in