Behind the paper: What comes after stable disease?
Published in Biomedical Research, General & Internal Medicine, and Pharmacy & Pharmacology
The first evaluation scan after starting anti-cancer therapy is a moment of high stakes. For patients with metastatic melanoma receiving therapy with anti-PD-1 inhibitors, this initial assessment can feel like a verdict, raising hopes for a durable response or confirming fear of progression. For clinicians, it’s the first opportunity to assess the effect of the therapy and to offer guidance based on this early result.
But not all outcomes are clear-cut. Using standard RECIST criteria, responses are grouped into complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). While CR and PR offer reassurance, and PD in most cases signals a need to change course, SD is a prognostic grey zone that can be frustrating for both patients and physicians. What does it mean when there is no clear shrinkage or growth of the cancer?
This question became the driving force behind our recent study, where we analyzed real-world data from 1,048 Danish patients with metastatic melanoma treated with pembrolizumab between 2014 and 2022. Our goal was to better understand what happens after initial SD and whether these patients can still obtain long-term benefit.
Why landmark analysis matters in observational research
Before diving into the results, we want to address an important methodological challenge: immortal time bias. This type of bias can occur in observational studies when group assignments are based on events happening later during follow-up. For example, if a patient with initial SD is classified based on eventually achieving CR, then they must have survived long enough to get there, thereby introducing a period of “immortality” to the analysis, which can skew survival comparisons.
To handle this, we used landmark analysis, a method that sets a fixed time point and then classifies patients based on their status at that point. In survival analysis, this approach helps ensure that everyone included can experience an event (progression or death) and that no one is “immortal”, providing a more accurate reflection of outcomes.
In this study, we chose a 4-month and a 12-month landmark. In the 4-month landmark analysis, we compared patients with early SD to patients with other responses, while the 12-month landmark enabled analysis of patients with initial SD and later response compared to patients remaining in SD or patients with initial response. This allowed us to compare survival outcomes in a way that minimized immortal time bias.
What we found: SD isn't the end of the story
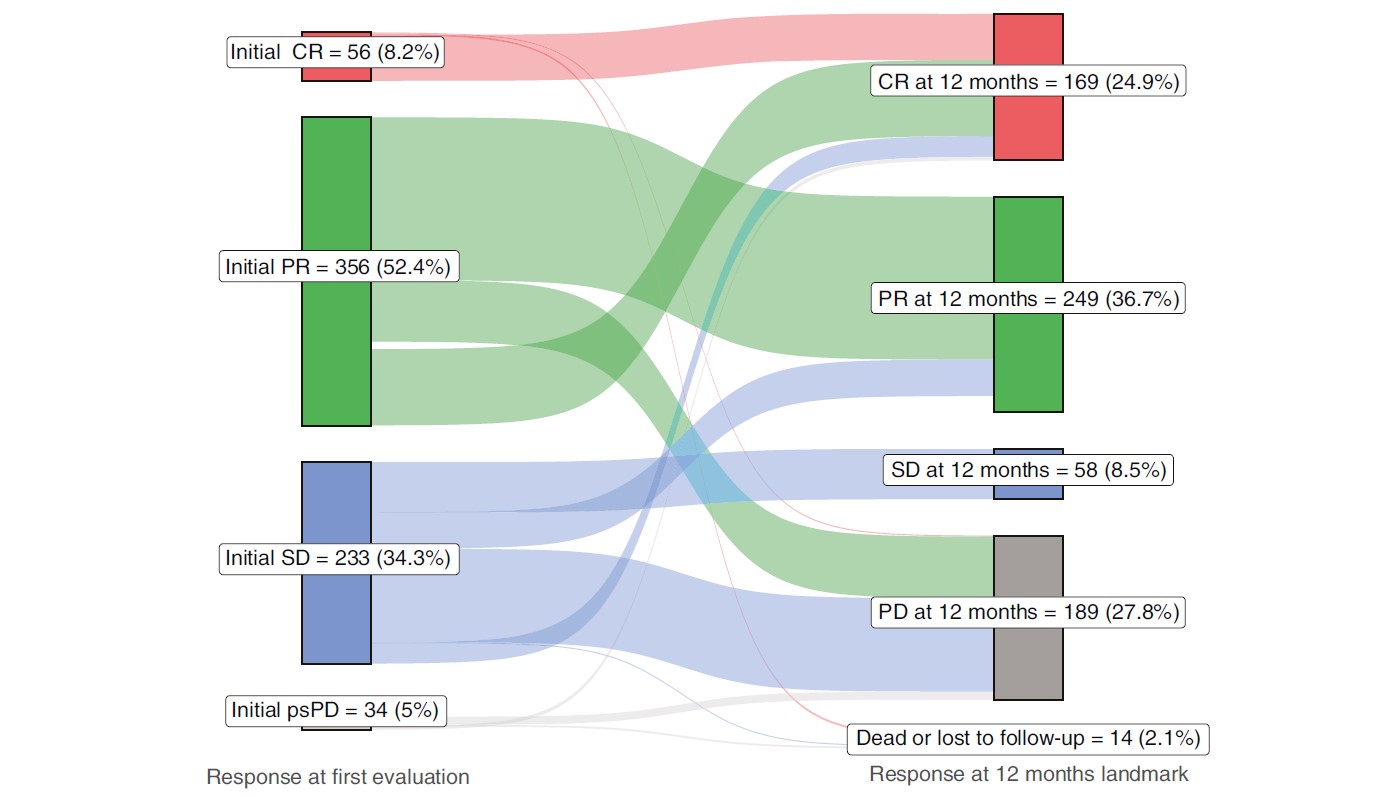
Out of the 1,048 patients, 233 (22%) had SD on their first evaluation scan. For many, this was just the beginning of a longer trajectory towards either response or progression, as 75% had changed their response status by the 12-month landmark (Figure 1).
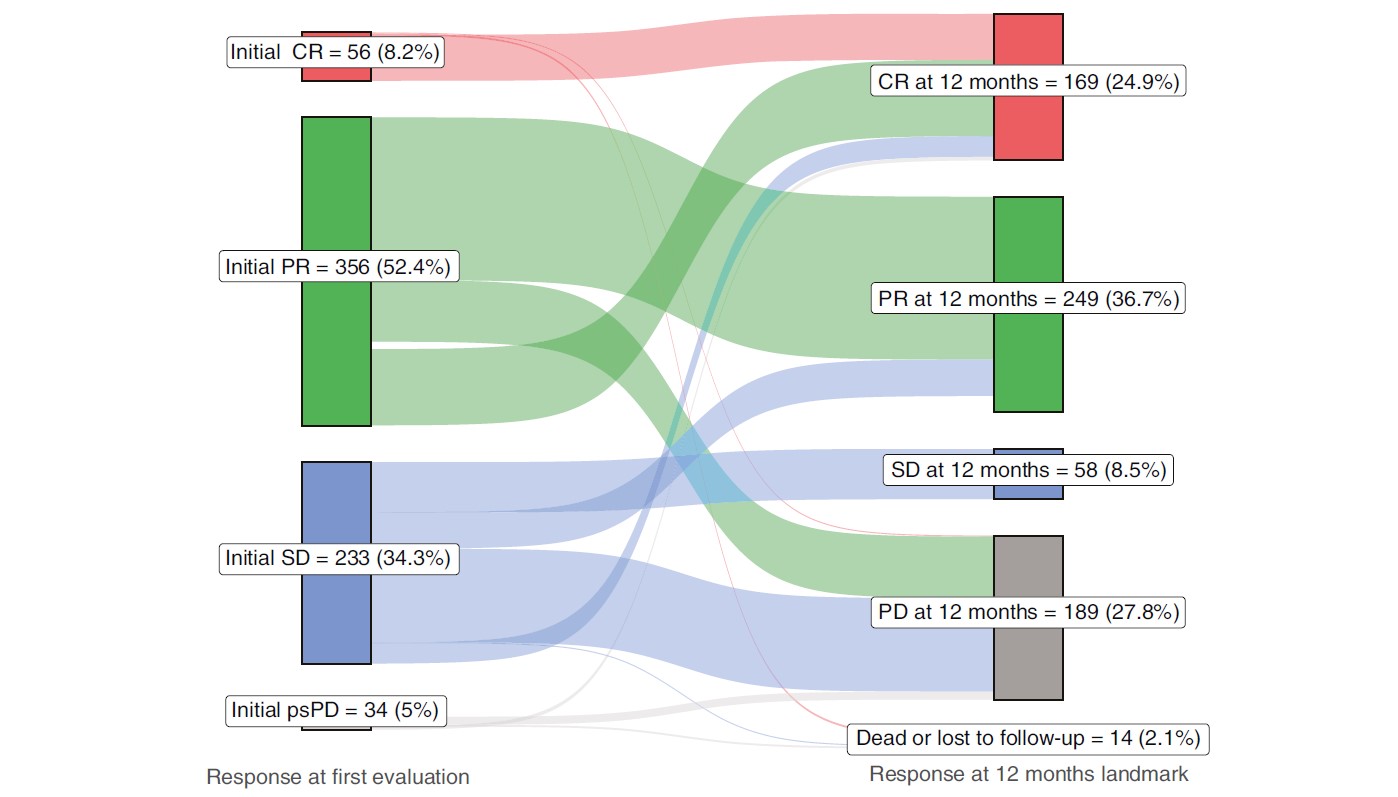
Figure 1: Change of response status from the first evaluation scan to the 12-month landmark.
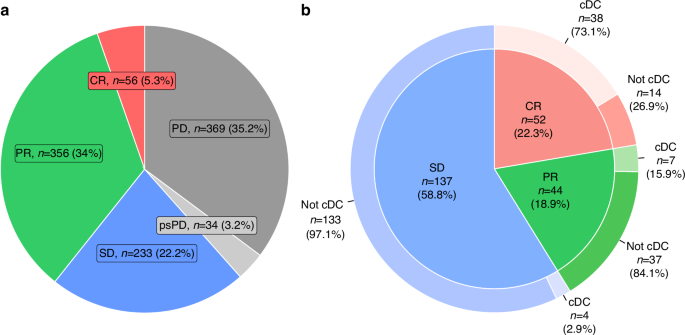
Encouragingly, nearly 40% of patients with initial SD eventually obtained an objective response, and over half of those achieved CR (Figure 2a, b). We also found that 20% of all patients with initial SD achieved continued disease control (cDC) (Figure 2b). These patients maintained a durable benefit from pembrolizumab with progression-free survival extending beyond two years.
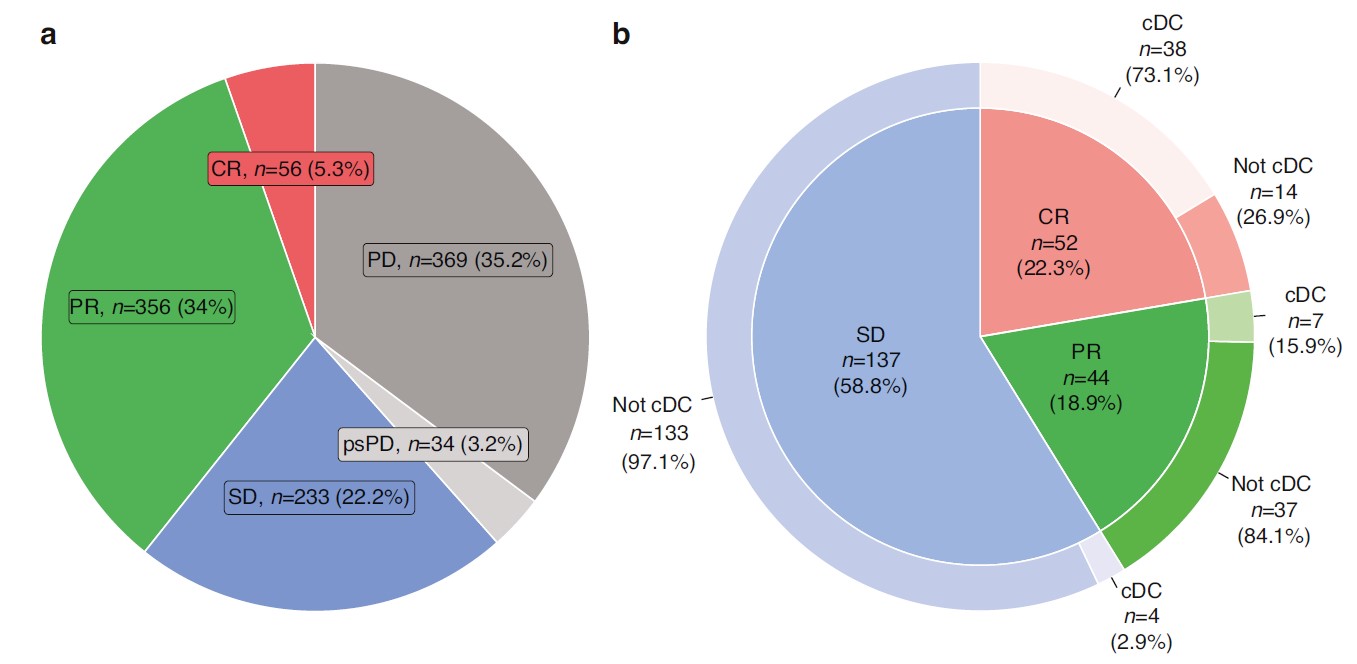
Figure 2: a, Distribution of the total population (n=1048) by response status at the first evaluation scan. b, Distribution of patients with initial SD (n=233) by the best overall response and achievement of continued disease control.
Interestingly, half of the patients with cDC discontinued their pembrolizumab treatment while still classified as SD, yet their disease remained controlled. This suggests that immune-mediated tumor suppression continues beyond visible response on imaging and that radiographic SD doesn’t always mean immunological inactivity.
Depth of later response matters
One of the most striking findings was the relationship between the depth of subsequent response and long-term outcomes. In a multivariable analysis comparing the patients who remained in SD to those who obtained a later response, we found that those who eventually achieved PR had half the risk of progression, while those who reached a CR had an 85% reduction in progression risk. Kaplan-Meier analysis, including landmark analysis, further underlined the advantageous prognosis of patients achieving subsequent CR (Figure 3a, b).
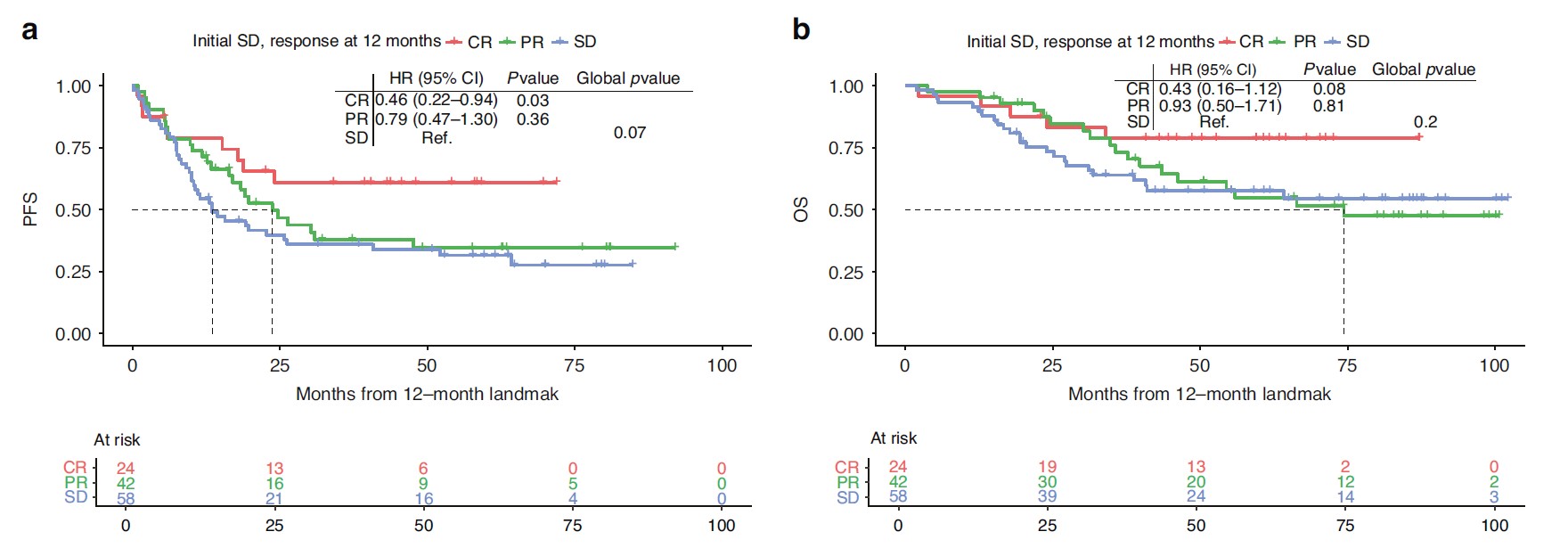
Figure 3: a, Progression-free survival of patients with initial SD stratified by response status at the 12-month landmark. b, Overall survival of patients with initial SD stratified by response status at the 12-month landmark.
Notably, patients with initial SD who transitioned to PR or CR by 12 months had survival outcomes comparable to those with initial PR or CR, respectively. This underlines that early SD is not necessarily a poor prognostic sign.
Who are the late responders?
To help distinguish patients likely to become late responders from those at higher risk of progression, we explored several baseline characteristics and biological markers as possible predictors. In a multivariable analysis, BRAF wildtype and PD-L1 expression ≥1% were both associated with improved progression-free survival. Conversely, advanced stage (M1d) and poorer performance status at baseline predicted worse overall survival.
We also looked at a subset of patients evaluated by FDG-PET/CT imaging. Among those with initial SD, patients who showed concomitant decreasing metabolic activity had a numerically lower risk of progression, suggesting a role for metabolic response as an early predictor of benefit, even when the CT scans are inconclusive.
Why this matters for patients and clinicians
Immunotherapy has fundamentally altered the treatment and prognosis of patients with melanoma and many other cancers. But the distinct kinetics and response patterns sometimes seen with immunotherapies demand a more nuanced interpretation of early imaging.
While a first scan showing SD may feel ambiguous, our findings suggest it should not necessarily be seen as discouraging. For many patients, SD marks the beginning of a path toward a response and even long-term control. As clinicians, being aware of the potential for delayed responses and predictors indicating either subsequent benefit or progression will be key to optimizing the treatment of these patients. Ultimately, we hope this work brings clarity to an uncertain early phase in the treatment of patients with melanoma and can help guide the shared decision-making between physicians and patients.
Read more in the British Journal of Cancer.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in