Beyond the Clot: Transauricular Vagus Nerve Stimulation in Hyperacute Stroke — A Conversation with Dr. Gareth Ackland
Published in General & Internal Medicine
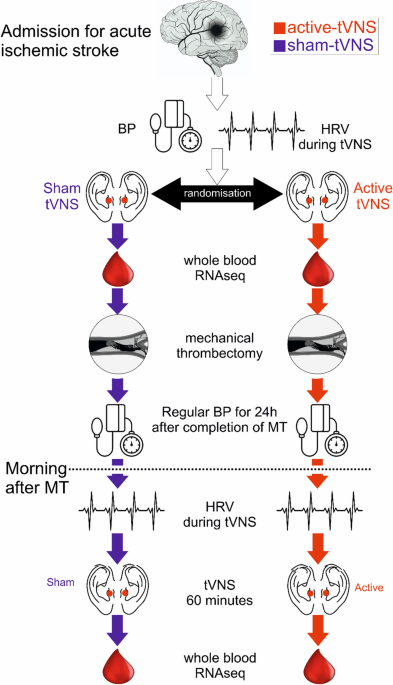
Mechanical thrombectomy has transformed acute stroke care, but recanalization does not address the autonomic and immune disturbances that follow reperfusion. In this phase 2 sham-controlled randomized trial (NCT05417009), Ackland and colleagues asked whether transcutaneous auricular vagus nerve stimulation (tVNS), delivered during and after thrombectomy, could reduce blood pressure variability and reverse early immunosuppression. The primary endpoint — coefficient of variation of systolic BP over 24 hours — was neutral, but exploratory HRV and whole-blood transcriptomic signals suggested a measurable biological effect. We invited Dr. Ackland to discuss the design, the results, and where the field should go next.
TSR: First, congratulations on this important study. What do you see as the central take-home message of this trial for the stroke field?
GA: Demonstrating feasibility and safety.
TSR: What motivated you to test tVNS in the hyperacute thrombectomy setting?
GA: Autonomic dysfunction is not only a dominant pathophysiologic feature of acute stroke, but potentially a therapeutic target. The focus has understandably been on “clot busting,” and rather less on the contribution of hemodynamic control.
TSR: What led you to focus on systolic blood pressure variability as the primary endpoint in this trial?
GA: Previous association studies identified this as a robust correlate of poorer outcomes, and it is also readily measurable from routinely collected data within EPRs.
TSR: The primary endpoint, systolic blood pressure variability over the first 24 hours, was neutral. How do you interpret that result in light of the accompanying changes in heart rate variability and whole-blood transcriptomic signals?
GA: First, this was a feasibility/safety study, so all the secondary outcomes reported are exploratory. Given the “pluripotent” therapeutic possibilities of the intervention, it is entirely possible that subclinical changes occur independent of the primary outcome. The disconnect between the two may reflect the secondary/exploratory outcomes being more sensitive biomarkers for the intervention, and an over-estimate of the possible separation in SBPV should that have occurred.
TSR: Looking ahead, what do you see as the most important next step for this line of work — refining stimulation timing and parameters, identifying the right biological responders, or moving toward imaging and functional outcomes such as edema, infarct evolution, and disability?
GA: If there is a role for modulating autonomic dysfunction, personalisation will likely be key. That may centre on stimulation timings, parameters (most likely frequency), and having a handle on acute versus chronic autonomic dysfunction in presenting patients. The likeliest target will be intermediate-term cardiovascular outcomes and restoring exercise capacity, both of which have a profound effect on the chances of recovery after stroke.
The full article, “Transauricular Vagus Nerve Stimulation in Acute Ischaemic Stroke Requiring Mechanical Thrombectomy: Sham-Controlled, Randomised Device Trial,” is published in Translational Stroke Research (2026) 17:10. doi: 10.1007/s12975-025-01404-7
Follow the Topic
-
Translational Stroke Research
A journal committed to the development of new strategies for prevention, assessment, treatment, and repair after stroke and neurotrauma.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in