Breaking the Mould: How LiverMultiScan is transforming MASLD diagnosis in a cost-effective way
Published in Healthcare & Nursing, Social Sciences, and Bioengineering & Biotechnology
Introduction
Have you ever wondered what the leading chronic liver disease is? Have you ever thought of its relationship with the development of liver cancer or its impact on the rates of liver transplantation? Steatotic liver disease, has been termed ‘the silent killer’ as most patients experience no symptoms, leaving them unaware of their condition. Currently, one in three adults has steatotic liver disease, a figure predicted to rise to one in two by 2050. With the increasing prevalence, steatotic liver disease related deaths are projected to rise by 178% by 2030, making this condition a leading cause of lost working years, second only to ischaemic heart disease.
The costs associated with managing steatotic liver disease are staggering, with direct annual medical expenses exceeding $103 billion in the US and €35 billion in Europe. Currently, liver biopsy is considered the reference standard for diagnosis and monitoring; however, its invasiveness, subjectivity and well‐recognised limitations mean that it is not a scalable solution. Patients are often averse to this procedure due to the associated pain and potential hospitalisation, which, coupled with the rising disease prevalence, poses a significant challenge for healthcare systems.
To address this global health issue, we urgently need improved diagnostic pathways that are safe, utilise accurate and scalable tests, enhance diagnosis rates, alleviate pressure on healthcare systems, and most importantly, place the patient at the heart of care while improving their quality of life. This need to improve patient outcomes is what sparked a journey to explore the cost-effectiveness of using MRI as part of routine care, a RADIcAL1 journey that would take us back to the future.

From conception to reality: designing a study for the future
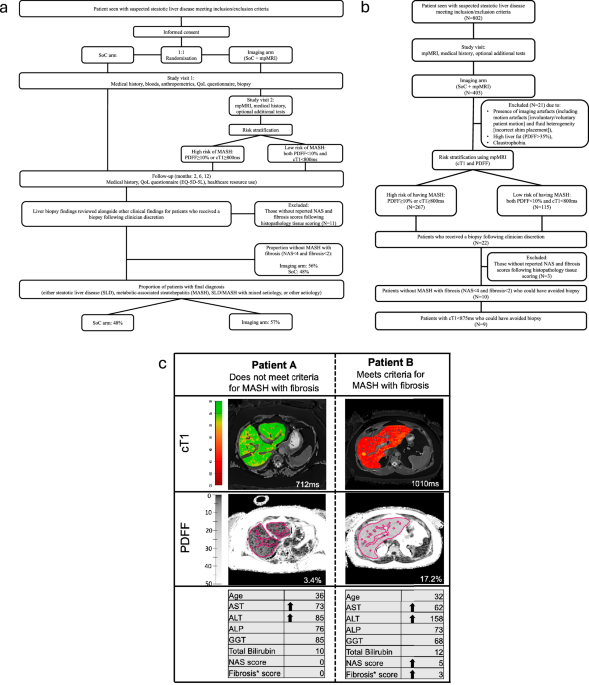
A decade ago, designing a study using MRI for diagnosis faced significant challenges. Diagnosis relied heavily on liver biopsy, patient management was even more varied than it is now, the disease was known as nonalcoholic fatty liver disease (NAFLD) rather than metabolic dysfunction-associated steatotic liver disease MASLD, and there was limited validation of MRI biomarkers in clinical care. Additionally, high costs and restricted access to advanced MRI technology hindered widespread adoption, while the absence of large-scale longitudinal data raised concerns about prognostic utility. Moreover, the lack of established reimbursement pathways for MRI-based diagnostics in MASLD further limited real-world feasibility. To put our best foot forward, we assembled a multidisciplinary team and convened a Delphi panel of clinicians, researchers, industry partners, biostatisticians, and other experts, all with the singular goal of designing an ambitious study to evaluate if MRI is a cost-effective, scalable, and clinically meaningful tool for MASLD diagnosis without compromising patient stratification.
Early days: wins, challenges, recruitment and expanding our reach
The early days brought unique challenges. We were launching a Horizon 2020 funded randomised control trial in four different sites from 4 different countries with 4 different ethical board and approval processes. This stage was full of wins and challenges making it both exciting and complicated. From selecting the right system to collect data accurately, to designing the system and making sure data were collected and entered correctly. As the study grew, we quickly realised two things: we needed to hire more staff to keep everything running smoothly, and we had to add more sites to meet our recruitment goals.
Running a study and navigating the pandemic
The Covid-19 pandemic was a challenging time which none of us will forget in a hurry. The pandemic changed the way studies were conducted. Different local and national restrictions meant we had to navigate and quickly adapt our methods to recruit and follow up with patients. With many patient visits moving online, MRI’s non-contact nature proved to be a significant advantage, allowing us to safely recruit the final patients while keeping the study on track. This period truly tested our team’s resilience and ability to adjust. The dedication and steadfastness of our collaborators needs to be commended and celebrated.
By the end of the study period, we had collected comprehensive data, including MRI scans, blood tests, biopsies, medical imaging, consultations, and questionnaires on healthcare resource use, at 2, 6, and 12 months from 802 participants successfully recruited across 10 sites in the UK, Germany, the Netherlands, and Portugal.
Assessing cost effectiveness
Just when we thought the hardest part was over, we were faced with a massive database and a complex data analysis plan to follow. Cleaning and organising the data was no easy task. With a solid statistical plan in hand, we began analysing both the clinical and economic data. Key decisions made years earlier now came into play. For example, when calculating MRI costs, we only counted the scan time, leaving out extra expenses like clinician and radiologist time, as well as hospital overheads; costs which are usually included in health economic assessments. Similarly, for patients who had liver biopsies, we did not factor in the costs of complications, which can include serious risks such as hospitalisation, major bleeding, or even death. Although this strict approach was challenging, it allowed us to evaluate the true cost-effectiveness of using MRI in patient care without worrying about the variability between sites, centres and countries resulting from the drastically different healthcare systems and standards of practice.
Why this matters
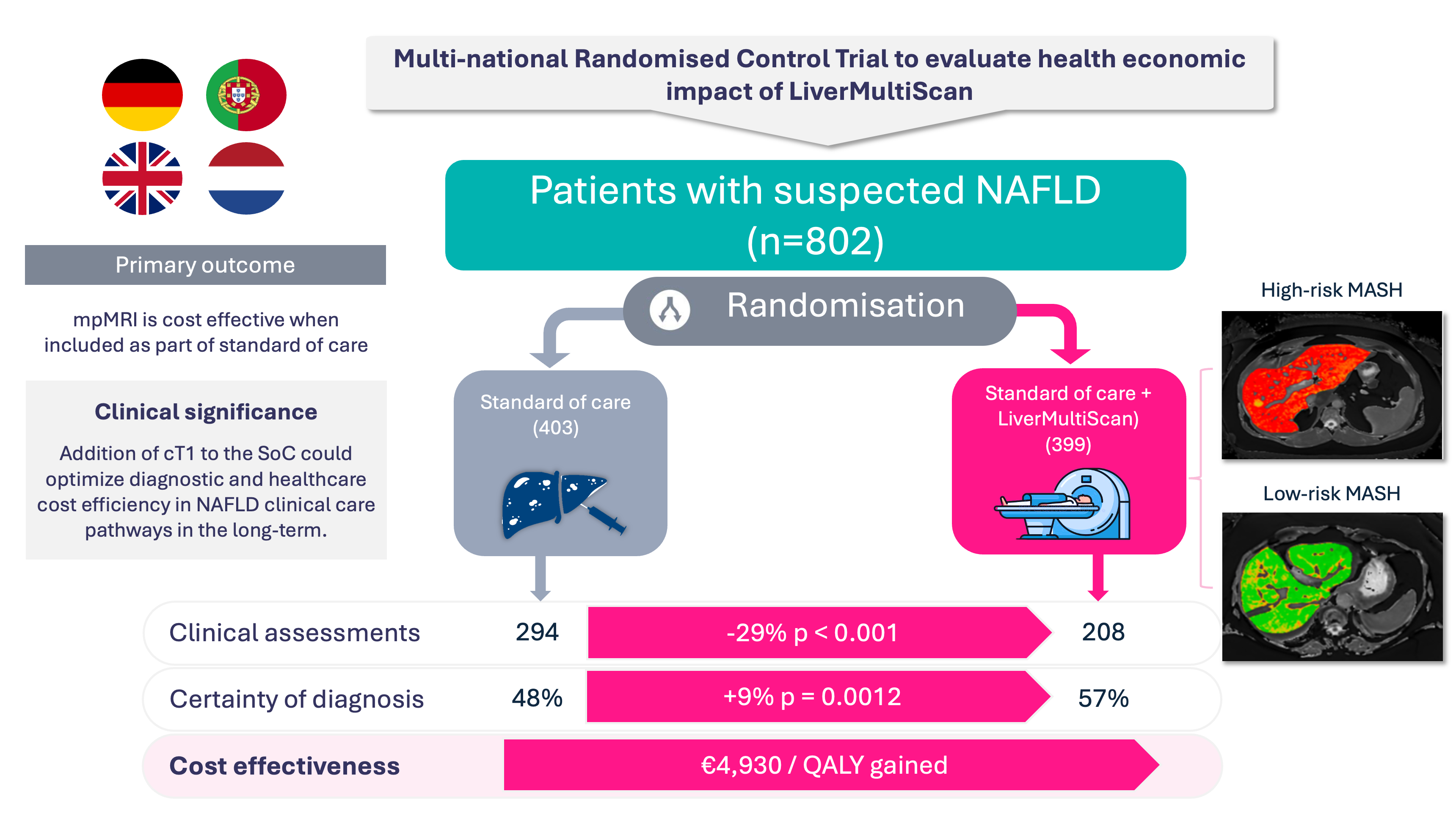
Our findings show that LiverMultiScan is a cost-effective tool with an ICER per QALY gained of €4,929.
For the non-health economist in the room, the Incremental Cost-Effectiveness Ratio (ICER) per Quality-Adjusted Life Year (QALY) is a tool used to measure the value of a healthcare intervention. It shows how much extra money is spent to gain one additional unit of health. In simpler terms, this means it helps us decide whether a new treatment is worth the extra cost based on the extra health benefits it provides. Currently, assessment bodies like (NICE) have set the threshold at £20,000 which means that even with our very stringent assessment criteria, the use of MRI is cost-effective with a ratio <20% of the accepted threshold.
Additionally, our findings showed that using LiverMultiScan improves diagnosis rates by ~10% (57% using LiverMultiScan vs 48% current standard-of-care), reduces the need for specialist consultations (7% less hospital appointments and visits to general practitioners (GPs), 29% less ultrasound procedures), and can be used to avoid 50% of unnecessary biopsies. This means that incorporating an MRI scan into routine care can lead to faster, more accurate, and less invasive diagnoses, without increasing overall healthcare costs. In places like the US and some parts of Europe and Asia, MRI is already being used as part of routine care, but we need to do more. Precision medicine, the right intervention for the right patient at the right time, is a goal every patient deserves. The vision and courage of our steering team in challenging the status quo in this rapidly changing field makes me truly proud to be a scientist

Looking back to look ahead: the future is now
As I look back over the past few years and I think about the hurdles we jumped over and the wins encapsulated in the 5,000 words making up our manuscript, I am reminded of the quote popularised by Sir Isaac Newton “[we are] standing on the shoulders of giants”. In the last 12months we have seen radical changes in nomenclature to reduce stigma and the first MASLD therapies being approved; a step that has brought renewed hope for patients with MASLD. Looking ahead, I’m excited to see the research and patient care landscape continue to grow. If research pioneered almost a decade ago can answer todays’ questions, with the knowledge and technology available today, I’m confident that by working together, scientists, doctors, engineers, patients, policymakers, regulators, clinical societies, industry partners and the community, we can continue to move the needle and make these breakthroughs accessible to everyone.
Follow the Topic
-
Communications Medicine
A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.

Related Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Jun 01, 2026
Public health and health governance in China
Publishing Model: Open Access
Deadline: Jul 31, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in