Clonal dynamics and stereo-seq resolve origin and phenotypic plasticity of adenosquamous carcinoma
Published in Cancer

Adenosquamous carcinoma (ASC) is a rare entity of non-small-cell lung cancer (NSCLC) with an incidence of 0.4% to 4% of all lung cancers1. It is characterized by a biphasic morphology containing at least 10% adenocarcinoma (AC) and squamous cell carcinoma (SCC) components2. Earlier studies showed that resected ASC was more aggressive and had a higher possibility of metastatic seeding than pure AC or SCC, resulting in a poor prognosis3–6. Several studies revealed that treating EGFR-mutant ASC with first- or third-generation TKIs produced similar efficacy as typical lung adenocarcinomas (LUAD)7–9.
Presenting mixed glandular and squamous phenotypes, how ASCs comes about remained mysterious. According to World Health Organization (WHO) Classification of Tumours, two potential pathogenetic mechanisms have been proposed: multipotent tissue stem cell origin10 and transdifferentiation from either AC or SCC11,12. Recent genomic studies of micro- or macro-dissected ASCs further revealed shared mutations between AC and SCC, including EGFR and KRAS, suggesting ASC are potentially monoclonal origin1,13,14. These studies primarily focused on hotspot mutations or used hotspot sequencing panels. Information from broader genomic areas is crucial in understanding the clonal relationships and evolutionary trajectories.
Study Design
Archived (formalin-fixed paraffin-embedded) FFPE samples from thirty-three patients diagnosed with primary lung ASC underwent surgical resection at Shanghai Chest Hospital between 2017 and 2019 were involved. Of these 33 patients, 14 had lymph node metastasis and three had multiple primary lesions of pure AC or SCC at diagnosis, which were surgically resected. Then, laser-capture microdissection (LCM) was performed on all ASC sample sections using the ArcturusXT™ LCM system (Applied Biosystems). Additionally, surgical samples from seven patients diagnosed with EGFR-mutant primary lung squamous carcinoma (LUSC) were collected. Whole-exome sequencing was performed on microdissected ASCs and EGFR-positive primary LUSCs. Then, mutational signature and copy number were analyzed. Clonal/subclonal architecture and tumor evolution were reconstructed. Then, stereo-sequencing were performed on one slide of ASC sample, and spatial profiling and trajectory analysis were performed. The xenograft model was developed using malignant tumor cells of an ASC patient that isolated from biopsied tumor tissue. To evaluate the efficacy of EGFR TKIs in EGFR-mutant lung cancer patients, we included 160 LUAD, 52 ASC, and 65 LUSC patients who were treated with any EGFR-TKI monotherapy or combination therapies in the clinic.
Results
Genomic landscape of micro-dissected primary ASCs
Activating EGFR mutations were found in 11/33 patients (33%), including five with exon 19 deletion, five with L858R, and one with L861Q. All patients, except one patient, carried EGFR mutations in both AC and SCC components. MET exon 14 skipping was identified in both components of five patients (5/33, 15%), which was more frequently observed than in pure LUAD15. Additionally, three patients (9%) harbored KRAS G12C/D mutations (one G12D found only in SCC) and one had ERBB2 exon 20 insertion in both AC and SCC. Other Ras-pathway genes, such as NF1 (6/33) and KIT (3/33), were also detected. In the PI3K pathway, mutations in PIK3CA and TSC2 were observed in four AC component (4/33, 12%) and slightly lower in SCC (6%).
Overall, genomic profiles were similar between AC and SCC components, and most tumors present shared driver and passenger mutations, indicating possible same genomic origins of AC and SCC components. For arm-level copy number alterations, SCC components demonstrated significant and marginal significant enrichment of chromosome 4p loss and 11q loss, respectively, whereas AC components showed enrichment of 16q amplification.
Genomic features of primary and metastatic ASCs
Genomic instability (measured by fraction of genome altered, FGA) and proportion of clonal and subclonal mutations (measured by intratumoral heterogeneity (ITH) score) in primary and metastatic tumors were compared. Significantly higher proportion of FGA in primary ASCs than lymph node or pleural metastases were observed. Tobacco smoking contributed to significantly higher proportion of mutations in EGFR-wildtype LUSCs than in EGFR-positive subtypes. Overall, EGFR-positive LUSCs presented similar mutation signature profiles and ITH to EGFR-positive ASCs.
Reconstruction of tumor evolution in ASCs
To further explore the evolution routes of ASC, we reconstructed phylogeny trees based on single-nucleotide variants and CNVs from primary and lymph node samples with the maximum parsimony approach. Among the study patients, 13 had lymph node (LN) or pleural metastases (PM) and phylogenetic distance of these metastases were found to be closer to the ASC component with same histology. In addition to supporting the monoclonal origination of AC and SCC components, these evolutionary architectures also implied that the two components might evolve separately.
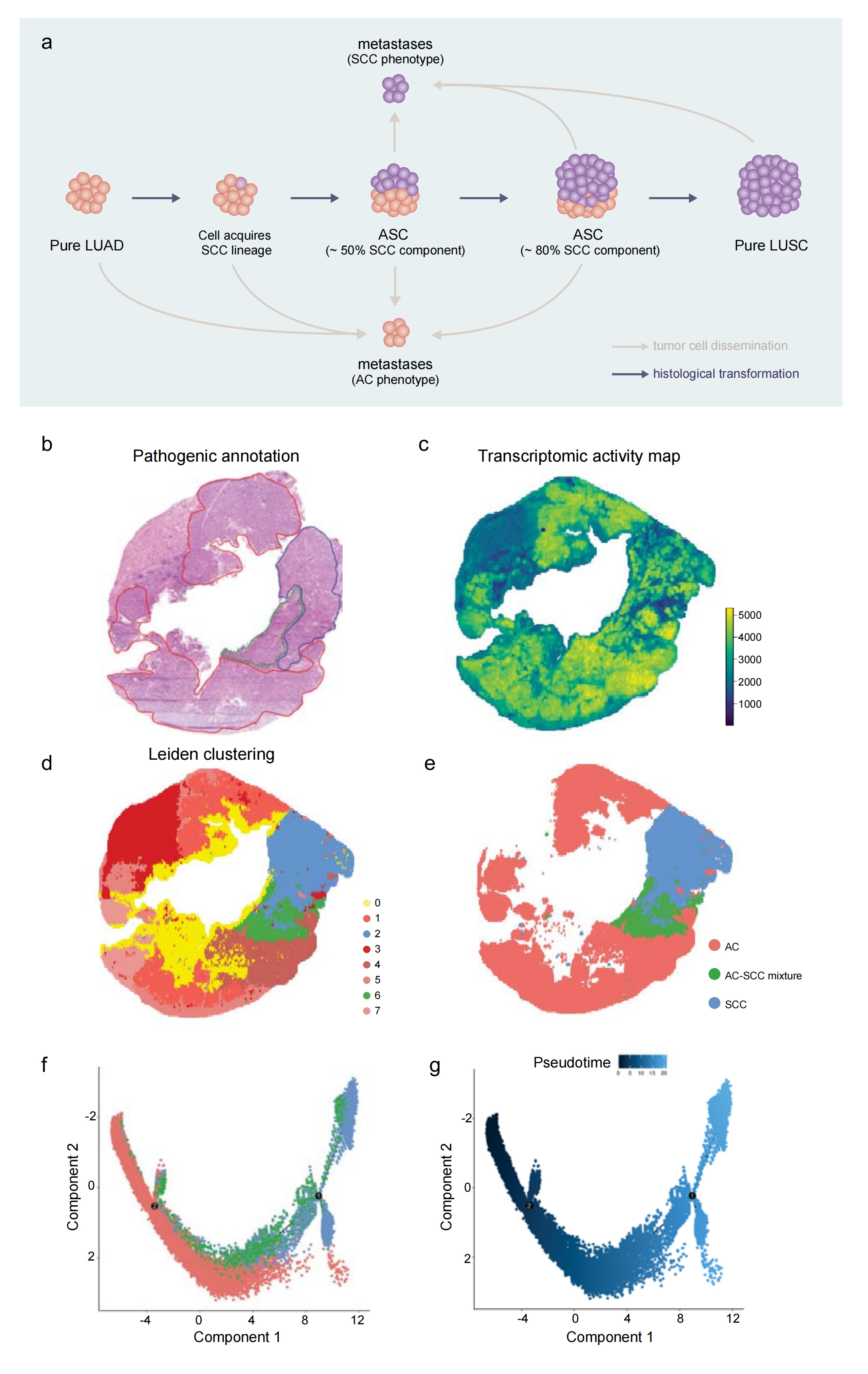
Deciphering dynamic transition between histological components in ASCs
Based on our genomic and phylogenetic evidence, we speculated that ASC was an intermediate state during potential transformation from AC to SCC. Different SCC proportion of ASC reported with clinical diagnosis of ASC then reflects the extend of squamous cell transition. To validate the evolutional concept between histomorphological components of AC and SCC, we applied Stereo-seq to obtain spatially resolved RNA profiles in 10μm tissue section from one prospectively collected resected ASC. Distribution of gene counts revealed higher transcription activity in AC areas than in SCC or AC-SCC mixture areas. Using phenotypic annotated clusters, we then constructed a transcriptional trajectory to elucidate the evolution path. The resulting trajectory showed AC and SCC formed two different branches, with the AC-SCC dual phenotype cluster located in between. Importantly, pseudo-time analysis elucidated the transition route from AC through dual phenotypes to SCC, supporting the proposed concept of ASC’s evolution direction.
Squamous transition observed in ASC-derived xenograft model
To further explore the phylogeny of ASC, patient-derived ASC cells were inoculated in female mice. Histology of tumors was compared before and after tumor inoculation. Both patient tissue and Passage 0 (P0) tumors showed strong diffuse expression of TTF1 and partial expression of P40 in different cell populations. Notably, starting from the P1 generation, TTF1 expression decreased markedly while P40 expression became more dominant. In P2, P3 and P4 tumors, there were hardly any TTF1 expressed. In contrast, more than 90% of the tumor regions were positive for P40, implying near-completion of squamous transition. Interestingly, no treatment was administered during the grafting and passaging processes, indicating that predetermined cell fates or natural selection forces driving histological transformation.
Efficacy of EGFR-TKIs in EGFR-mutant LUADs, ASCs and LUSCs
As approximately 30% of ASCs are EGFR-positive, we wondered how they respond to EGFR-TKIs especially in comparison to EGFR-positive ADCs and EGFR-positive LUSCs. Overall, the efficacy of EGFR-TKIs was similar among three subtypes, and the proportion of SCC components in ASCs did not significantly affect TKI efficacy.
In conclusion, we have found that AC and SCC components of ASC share similar mutational and copy number alteration profiles. By phylogenetic analyses, we confirmed that these components shared clonal origins and could disseminate separately during tumor evolution. We also demonstrated the histological transformation of ASC into squamous phenotype, suggesting that driver-positive LUSCs could originate from AC cells. In the clinic, EGFR-positive LUSC patients have benefited from first-line TKI treatment, highlighting the importance of molecular testing in all lung cancer subtypes to facilitate decision-making.
Reference
- Krause, A. et al.Deciphering the clonal relationship between glandular and squamous components in adenosquamous carcinoma of the lung using whole exome sequencing. Lung Cancer150, 132–138 (2020).
- Travis, W. D. et al.The 2015 World Health Organization Classification of Lung Tumors. J Thorac Oncol10, 1243–1260 (2015).
- Riquet, M. et al.Do patients with adenosquamous carcinoma of the lung need a more aggressive approach? J Thorac Cardiovasc Surg122, 618–619 (2001).
- Gawrychowski, J., Brulinski, K., Malinowski, E. & Papla, B. Prognosis and survival after radical resection of primary adenosquamous lung carcinoma. European Journal of Cardio-Thoracic Surgery27, 686–692 (2005).
- Maeda, H. et al.Adenosquamous carcinoma of the lung: surgical results as compared with squamous cell and adenocarcinoma cases. European Journal of Cardio-Thoracic Surgery41, 357–361 (2012).
- Mordant, P. et al.Adenosquamous carcinoma of the lung: surgical management, pathologic characteristics, and prognostic implications. Ann Thorac Surg95, 1189–1195 (2013).
- Hu, M. et al.Clinical Outcomes of Different Generations of EGFR Tyrosine Kinase Inhibitors in Advanced Lung Adenosquamous Carcinoma. Mol Diagn Ther23, 773–779 (2019).
- Fan, L. et al.Clinical outcomes of epidermal growth factor receptor tyrosine kinase inhibitors in recurrent adenosquamous carcinoma of the lung after resection. Onco Targets Ther10, 239–245 (2017).
- Tochigi, N., Dacic, S., Nikiforova, M., Cieply, K. M. & Yousem, S. A. Adenosquamous carcinoma of the lung: a microdissection study of KRAS and EGFR mutational and amplification status in a western patient population. Am J Clin Pathol135, 783–789 (2011).
- Mather JP, et al.Isolation of cancer stem like cells from human adenosquamous carcinoma of the lung supports a monoclonal origin from a multipotential tissue stem cell. PLoS One. 2013 Dec 4;8(12):e79456.
- Kong M, Sung JY, Lee SH. Osimertinib for Secondary T790M-Mutation-Positive Squamous Cell Carcinoma Transformation After Afatinib Failure. J Thorac Oncol. 2018 Dec;13(12):e252-e254.
- Han X, et al.Transdifferentiation of lung adenocarcinoma in mice with Lkb1 deficiency to squamous cell carcinoma. Nat Commun.2014;5:3261.
- Lin, G. et al.Genomic origin and EGFR-TKI treatments of pulmonary adenosquamous carcinoma. Ann Oncol31, 517–524 (2020).
- Kang, S. M. et al.Identical epidermal growth factor receptor mutations in adenocarcinomatous and squamous cell carcinomatous components of adenosquamous carcinoma of the lung. Cancer109, 581–587 (2007).
- The Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature511, 543–550 (2014).
Follow the Topic
-
npj Precision Oncology
An international, peer-reviewed journal committed to publishing cutting-edge scientific research in all aspects of precision oncology from basic science to translational applications to clinical medicine.

Related Collections
With Collections, you can get published faster and increase your visibility.
Minimal Residual Disease and Circulating Tumor DNA Dynamics in Personalized Cancer Treatment
Publishing Model: Open Access
Deadline: Mar 12, 2027
Genomic Instability
Publishing Model: Open Access
Deadline: Jun 24, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in