Cranial Neuropathy as an Isolated Presentation of COVID-19: Evidence for Direct Neuroinvasion
Published in Neuroscience and Biomedical Research
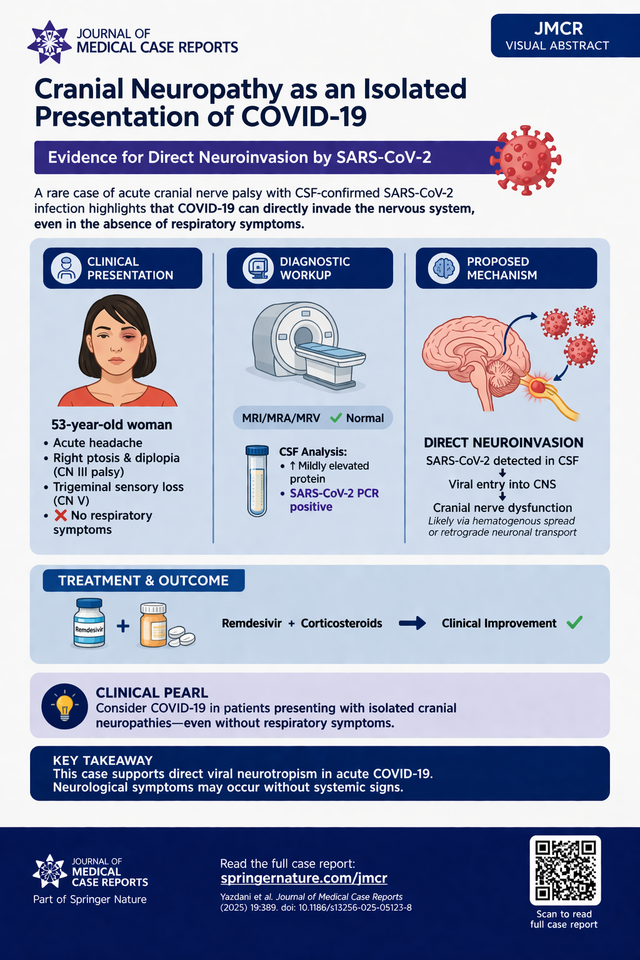

Neurological manifestations of coronavirus disease 2019 (COVID-19) are now well recognized, ranging from mild symptoms such as anosmia to severe complications including stroke and encephalopathy. However, cranial neuropathies are typically described as post-infectious, immune-mediated phenomena—most notably in the context of Miller Fisher syndrome or Guillain–Barré variants. This case report from the Journal of Medical Case Reports highlights a distinctly different mechanism: cranial neuropathy occurring during the acute infectious phase with direct viral detection in cerebrospinal fluid (CSF) .
A 53-year-old woman presented with acute headache, right ptosis, diplopia, and trigeminal sensory loss, notably without any respiratory or systemic COVID-19 symptoms. Neurologic examination localized deficits to cranial nerves III and V, raising concern for vascular, infectious, or cavernous sinus pathology.
Extensive neuroimaging—including MRI, MRA, and MRV—was unrevealing. However, SARS-CoV-2 PCR testing returned positive in both nasopharyngeal and CSF samples, a rare and critical finding. CSF analysis showed mildly elevated protein but no pleocytosis, and there was no radiographic or clinical evidence of alternative etiologies.
The patient was treated with remdesivir and corticosteroids, with subsequent improvement in cranial neuropathy.
This case is notable for several reasons:
Absence of respiratory symptoms, emphasizing atypical presentations
Concurrent CSF positivity, supporting direct viral neuroinvasion
Isolated cranial neuropathy, rather than typical post-infectious syndromes
While most neurological complications of COVID-19 are thought to be immune-mediated, this case supports multiple potential mechanisms, including:
Direct viral invasion of neural tissue
Immune-mediated neuronal injury
Microvascular dysfunction (especially relevant given comorbid diabetes)
Importantly, the detection of SARS-CoV-2 in CSF strongly favors true neurotropism, rather than secondary immune effects alone .
Clinical Take-Home Message (Pearl):
COVID-19 should be considered in patients presenting with acute cranial neuropathies—even in the absence of respiratory symptoms—particularly when diagnostic workup is otherwise unrevealing.
Question:
What is the most likely mechanism explaining cranial neuropathy in this patient?
A. Post-infectious autoimmune demyelination (Miller Fisher syndrome)
B. Microvascular ischemia from diabetes alone
C. Direct viral invasion of cranial nerves by SARS-CoV-2
D. Medication-induced cranial neuropathy
Correct Answer:
C. Direct viral invasion of cranial nerves by SARS-CoV-2
The key distinguishing feature in this case is the presence of SARS-CoV-2 RNA in the cerebrospinal fluid, which is rarely demonstrated in COVID-19 neurological syndromes. This finding supports direct neuroinvasion, likely via hematogenous spread or retrograde neuronal transport. While immune-mediated mechanisms (e.g., molecular mimicry) are more commonly implicated in COVID-19–related neuropathies, they typically occur days to weeks after infection and are not associated with viral detection in CSF. In contrast, this case demonstrates acute-phase neurological involvement with virologic confirmation, making direct viral toxicity the most plausible mechanism.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports

This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in