Decoding Cutaneous Gamma Delta T Cell Lymphomas
Published in Cancer
Gamma delta T cell lymphomas of the skin (CGDTLs) are highly aggressive lymphomas of the skin-homing gamma delta T cell. Previously, there had been no data to support current disease diagnoses, classification, and treatment strategies.
Two medical students at Northwestern, Jay Daniels (twitter: @Jay__Daniels; pictured left) and Peter Doukas (twitter: @petergdoukas; pictured right), sought to overcome this gap in knowledge. Peter compiled 42 of these otherwise uncommon cases. Jay elucidated their molecular bases. Through creativity, serendipity, and hard work, together they uncovered 1) the clinical manifestations of this disease, 2) the major drivers of disease heterogeneity, and 3) the genetic bases of this disease. Collectively, this work introduces a new framework for disease classification that will be pivotal for improved disease diagnosis, staging, and future clinical trials.

The most important take home finding of this study was that the phenotypic variants of CGDTLs reflect the the different gamma delta T cell subtypes that are present in human skin. By identifying the cellular origins of these CGDTLs, Jay uncovered novel gamma delta T cell subtypes, specifically the V gamma 3 (Vg3) V delta 2 (Vd2) cell founding the subcutaneous fat. Details below!
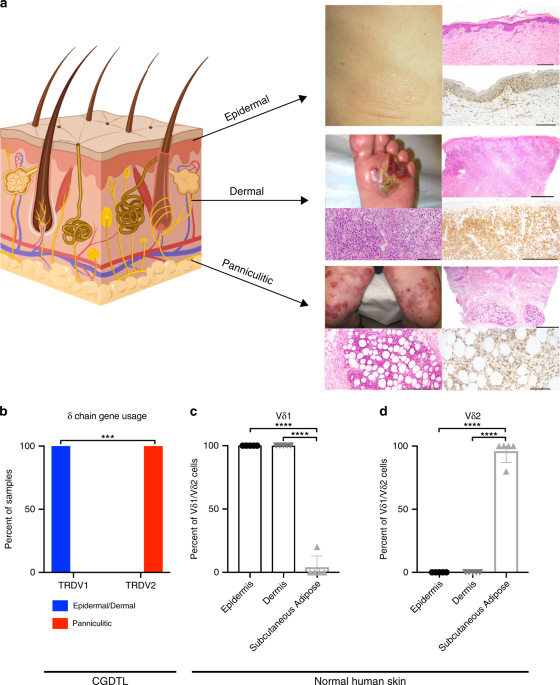
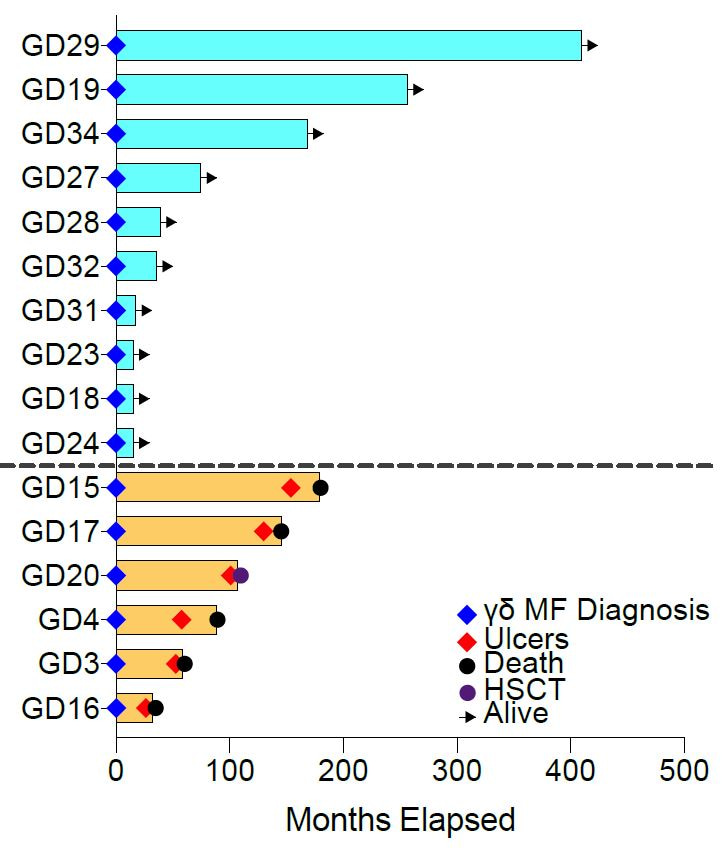
Peter first assembled 42 cases of CGDTLs, the second largest cohort of its kind. During clinical annotation, he discovered that CGDTLs are highly heterogeneous. They can present in any of the three major layers of the skin: epidermis, dermis and subcutaneous adipose tissue. Superficial, epidermal infiltrates present as thin patches and plaques and are associated with a mixed prognosis. Deeper infiltrates in the dermis or fat present as nodules and are associated with near-uniformly fatal outcomes.
Because of this disease heterogeneity, Jay wanted to confirm the diagnoses via close examination of the gamma delta T cell receptor sequences. He thought it would be useful to confirm the cell of origin and assess the tumor purity. Strikingly, he found that all of the lymphomas of the epidermis and dermis are derived from the V delta 1 (Vd1) gamma delta T cell. In contrast, all of the panniculitic cases (centered in the subcutaneous fat) are derived from the Vd2 gamma delta T cell.
The T cell receptor for gamma delta T cells often determines tissue homing and cellular functions. The vast majority of circulating gamma delta T cells in the blood are V gamma 9 V delta 2. It is thought that the gamma delta T cells in the mucosa are typically Vd1.
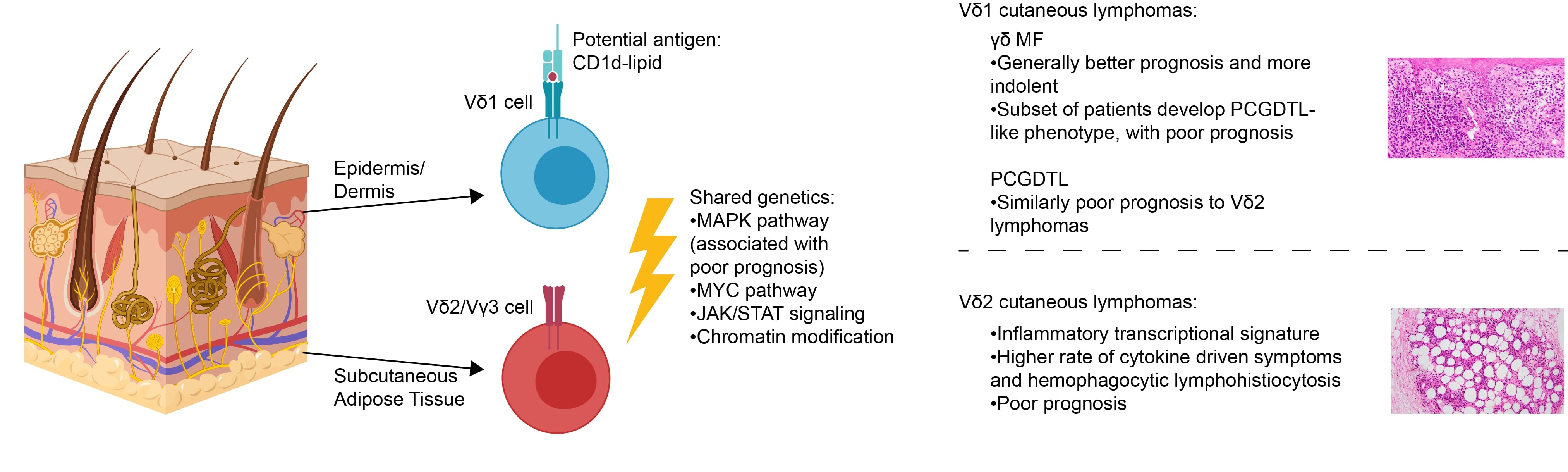
Jay hypothesized that these cells reflected the skin-homing gamma delta T cell in each skin compartment. Indeed, in non-diseased human skin, nearly all of the gamma delta T cells in the epidermis and dermis express the Vd1 receptor. In contrast, nearly all of the gamma delta T cells in the subcutaneous fat all express the Vg3 Vd2 receptor. In other words, by studying gamma delta T cell lymphomas, Jay uncovered an underappreciated cell type in the subcutaneous fat.
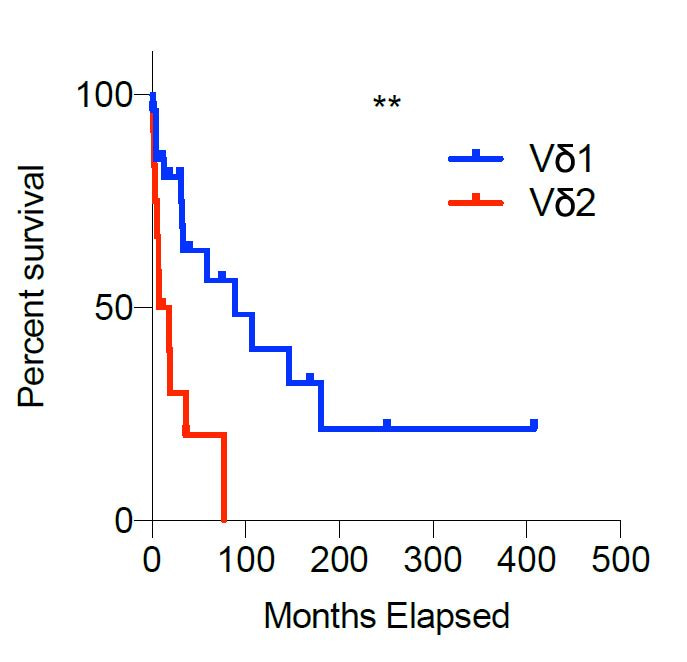
Moreover, the cell of origin determines clinical behavior and prognosis. Overall, the median survival is 12.75 months in Vd2 lymphomas, a fraction of the median survival in the Vd1 cases (89 months, P value < 0.005; log-rank test).
Moreover, the Vd1 and Vd2 lymphomas are transcriptionally distinct. The Vd2 lymphomas express higher amounts of mRNAs that correspond to cytotoxic proteins and cytokines. Correspondingly, Vd2 lymphomas are more likely to present with abnormal lymph nodes, cytokine-related paraneoplastic syndromes (such as hemophagocytic lymphohistiocytosis), and clinical features of cytotoxicity. Although rates of metastasis are similar between either group, involvement of the gut epithelium (a site normally populated by Vd1 cells) is exclusively found in the Vd1 lymphomas.
These unique cells of origin drive both overall clinical presentation and prognosis. Vd1 lymphomas are more likely to present with patches and plaques for cutaneous lesions, whereas Vd2 lymphomas prefer ulcerated, tumor lesions. Features such as abnormal lymph nodes and systemic cytokine storm are also more common in the Vd2 phenotype. This factor owes to the transcriptionally distinct nature of Vd1 and Vd2 CGDTLs, with the latter favoring greater amounts of mRNAs that correspond to cytotoxic proteins and cytokines.
Our findings have important implications for disease classification. Currently, gamma delta lymphomas of the skin are classified as either gamma delta mycosis fungoides (GDMF) and primary cutaneous gamma delta T cell lymphomas (PCGDTLs). GDMF and PCGDTLs are currently considered distinct diagnoses with disparate prognoses. GDMFs are considered indolent whereas PCGDTLs are considered universally fatal.
Our data suggests they are part of a disease spectrum. GDMF and epidermal/dermal PCGDTLs share the same cells of origin. Moreover, their clinical presentations can overlap. The majority of our GDMFs are indolent, however a subset display a phenotypic switch. They thus acquire the clinical, genetic, and molecular features of PCGDTLs and become universally aggressive. All cases died of disease or underwent allogeneic hematopoietic stem cell transplantation (HSCT), displaying a median survival of 16.5 months after the phenotypic switch.
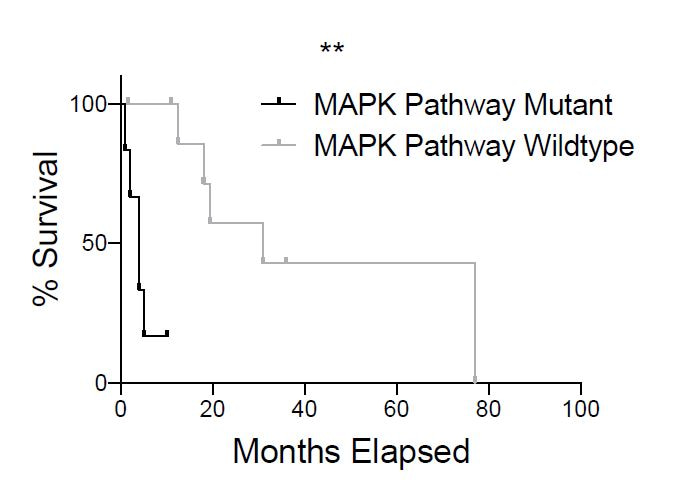
Lastly, driver genes that may play a key role in the pathogenesis of CGDTL were identified. Abnormalities in important signaling pathways were frequently noted, including mutations in the MAPK, MYC, and JAK/STAT signaling pathways. These mutations have clinical implications, including worse survival in patients with MAPK pathway mutations (P value < 0.005; log-rank test) and several mutations that have been targeted with specific drugs in other cancer types. Interestingly, there are no statistically significant difference in genetic drivers between the Vd1 and Vd2 CGDTLs.
Overall, this work paves the way for new approaches to thinking about the classification, origins, and therapies going forward for this rare and aggressive disease.
Follow the Topic
-
Nature Communications

An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.
Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Advances in neurodegenerative diseases
Publishing Model: Hybrid
Deadline: Mar 24, 2026




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in
Great work - thank you for your contribution to understanding this challenging disease.