Evaluating pneumococcal memory B cells in a low- and middle-income setting and the important role of capacity building
Published in Immunology
Children in low- and middle-income countries (LMICs) are disproportionately affected by lower respiratory tract infections, with an estimated 650,000 deaths occurring in children under five years old each year and more than half of these due to pneumonia. Safe and effective pneumococcal conjugate vaccines (PCVs) are available, but many children in high disease burden countries are unable to access these vaccines due to their high costs. Fewer doses, if it works, may improve vaccine access.
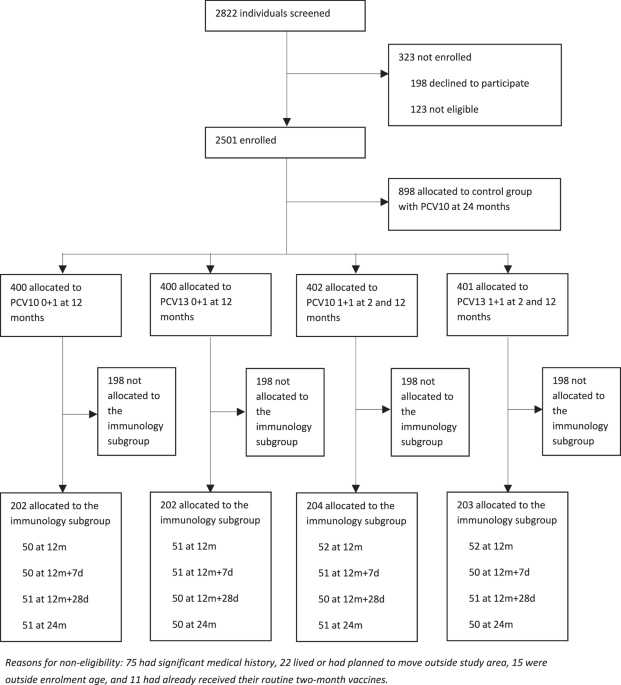
We conducted a randomised controlled trial in Viet Nam to understand if one or two doses of 10- or 13-valent PCVs (PCV10 or PCV13) provides similar protection as three doses currently recommended by the World Health Organisation. Our main study enrolled 2501 infants and found that a two dose PCV schedule (one primary and one booster dose) greatly reduced vaccine-type pneumococcal carriage (a precursor for pneumococcal disease). The schedule also induced robust immunogenicity, characterised by pneumococcal serotype-specific IgG antibody concentrations and opsonophagocytic titres (measuring functional capacity of antibodies).
These two immunological measures are considered gold-standard by regulatory agencies to determine immunogenicity. However, antibody concentrations often wane rapidly, which limits the ability to predict long-term protection against pneumococcal carriage and disease such as pneumonia. Despite these waning antibody levels in the months post vaccination, we know that protection against carriage and disease is generally maintained for longer. This suggests that other protective immune markers are likely to be important, but which have yet to be identified or validated in larger studies .
In recent years, there has been a great deal of interest in whether memory B cells (Bmem) might be a more reliable marker of long-term protection following PCV. As part of the trial, we examined Bmem dynamics in infants who received one or two doses of PCV up to 12 months post-vaccination, including an important seven-day post-vaccination timepoint which is not commonly measured in other Bmem studies. Our recently published study of 811 infants found that serotype-specific Bmem levels peaked seven days post-vaccination, which is faster than IgG levels that peaked one-month post-vaccination. We observed greater serotype-specific Bmem numbers for the two-dose compared to one dose schedule and for PCV13 compared to PCV10. Importantly, we found that Bmem numbers did not wane as rapidly as IgG levels by 12 months post-vaccination, highlighting the potential utility of Bmem in predicting long-term protection.
Our trial was the first to assess Bmem levels in infants following reduced-dose PCV schedules in an LMIC setting, where the disease burden is the highest. While many studies have examined Bmem responses to PCV, this is the first such study to look at these responses in a setting with high pneumococcal exposure and where PCV is not currently used. As such, this study provided a unique opportunity to examine the relationship between different immune components and susceptibility to carriage.
Local capacity building was the key to success
The success of this trial and the Bmem results was due to many factors, including the high level of engagement and trust between study staff and participant families and the highly skilled expertise of local laboratory staff based at the Pasteur Institute of Ho Chi Minh City (PI-HCMC), Viet Nam, where this study was conducted. The latter point is important, since local capacity building is critical to long-term sustainability of research to improve health outcomes. In the years leading up to the trial, a significant amount of effort was invested by both staff in Viet Nam and the Murdoch Children’s Research Institute (MCRI) in Melbourne, Australia, to establish local laboratory facilities and expertise. This involved visits by Vietnamese scientists to MCRI as well as several visits to PI-HCMC by the MCRI team for laboratory training. This led to the establishment of laboratory expertise in the conduct of both WHO pneumococcal serotype-specific IgG ELISA and pneumococcal Bmem method.
For this study, we wanted to undertake Bmem assays on freshly isolated peripheral blood mononuclear cells (PBMCs) in order to maximise the quality and robustness of the data. This presented a challenge as we needed to have a separate cell culture facility that had all the necessary equipment, such as class II biohazard hoods, CO2 incubators, microscopes and centrifuges. We also needed to establish a liquid nitrogen storage facility that allowed us to cryopreserve any remaining PBMCs from the study samples. After an intensive series of training exercises, the local study team built the capacity and expertise for daily and immediate processing of blood samples. Once completed, the assay plates were stored and then shipped to MCRI where they could be analysed on an automated plate counter. Frequent and effective communication between the PI-HCMC and MCRI teams played a critical role in this highly successful model, as we could identify and resolve any technical issues rapidly. The quality of the study results is a testament to the strong collaboration and hard work, particularly by the scientists in PI-HCMC, over a period of 16 months.
Looking ahead
Findings from our main trial suggest that a two-dose schedule is suitable as a transition from mature PCV programs or for new introductions in conjunction with a catch-up campaign. On the other hand, a one-dose PCV schedule also had some effect on carriage and generated a reasonable immune response but may be more suitable for humanitarian or remote settings. The data generated from this immunological study will inform ongoing studies aimed at addressing the correlates of protection for pneumococcal carriage, which will ultimately provide children in LMICs with greater protection from invasive pneumococcal diseases. This remains an important research gap and our trial site and study outcomes are well-positioned to make significant contributions in this area. The overall success of this program, funded by the Australian Government and the Bill & Melinda Gates Foundation, has allowed the team at PI-HCMC to establish a cutting-edge facility to study cellular immune responses. This is not limited to PCV but could potentially be used for other infectious diseases and vaccines of relevance to the region. The MCRI team have ongoing collaborations with the PI-HCMC team in a number of different areas, including HPV and measles, which have been possible due to this success.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Ask the Editor - Immunology, Pathogenesis, Inflammation and Innate Immunity
Got a question for the editor about the complement system in health and disease? Ask it here!
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Biosensing
Publishing Model: Hybrid
Deadline: Sep 30, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in