JMCR: Clinical Reasoning From Case Reports
Published in Neuroscience and Biomedical Research
Explore the Research
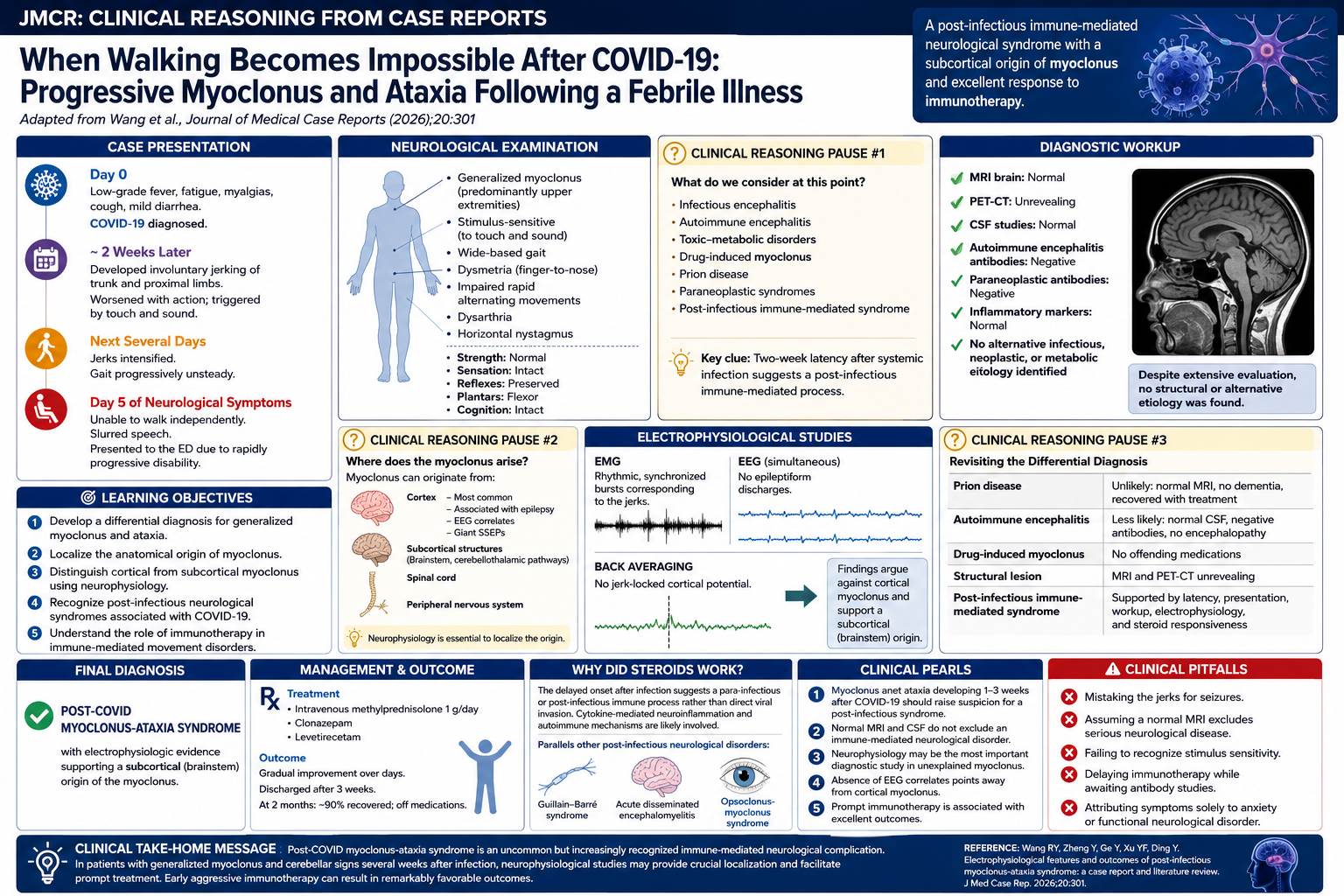
Electrophysiological features and outcomes of post-infectious myoclonus-ataxia syndrome: a case report and literature review
Introduction
COVID-19 has expanded the spectrum of post-infectious neurological syndromes. While Guillain–Barré syndrome and encephalitis are well recognized, movement disorders remain comparatively uncommon. Among these, the combination of generalized myoclonus and cerebellar ataxia represents a particularly distinctive syndrome.
The following case illustrates how careful localization and neurophysiologic testing can reveal the origin of myoclonus and guide effective immunotherapy.
Learning Objectives
After completing this exercise, readers should be able to:
- Develop a differential diagnosis for acute generalized myoclonus.
- Recognize the clinical features of post-infectious myoclonus-ataxia syndrome.
- Localize myoclonus anatomically using neurophysiology.
- Distinguish cortical from subcortical myoclonus.
- Understand the rationale for immunotherapy in post-COVID neurological syndromes.
Case Presentation
A 52-year-old woman developed low-grade fever, fatigue, myalgias, mild diarrhea, and cough. COVID-19 was diagnosed and treated symptomatically.
Two weeks later, she noticed involuntary jerking movements involving her trunk and proximal limbs. The movements worsened with action and were triggered by tactile and auditory stimuli. Her gait became increasingly unsteady.
Over several days, the jerks intensified. By the fifth day of neurological symptoms, she had become unable to walk independently and developed slurred speech. She presented to the emergency department because of rapidly progressive disability.
Clinical Reasoning Pause
The combination of:
- Acute to subacute progression
- Stimulus-sensitive generalized myoclonus
- Ataxia
- Dysarthria
raises several possibilities:
Infectious encephalitis
Autoimmune encephalitis
Toxic-metabolic disorders
Drug-induced myoclonus
Prion disease
Paraneoplastic syndromes
Post-infectious immune-mediated syndrome
The two-week interval after systemic infection is particularly suggestive of a post-infectious process.
Neurological Examination
The patient demonstrated:
- Generalized myoclonus involving predominantly the upper extremities
- Wide-based gait
- Dysmetria during finger-to-nose testing
- Impaired rapid alternating movements
- Dysarthria
- Horizontal nystagmus
Importantly:
- Strength was normal.
- Sensory examination was normal.
- Reflexes were preserved.
- Plantar responses were flexor.
- Cognitive function was intact.
Localization
The coexistence of:
- Dysmetria
- Nystagmus
- Ataxia
- Dysarthria
strongly implicates cerebellar pathways.
The stimulus-sensitive generalized myoclonus suggests involvement somewhere along the cortical-subcortical-brainstem motor network.
The next question becomes:
Where does the myoclonus originate?
Clinical Reasoning Pause
Myoclonus can arise from:
Cortex
- Most common
- Often associated with epilepsy
- Giant somatosensory evoked potentials
- EEG correlates
Subcortical structures
- Brainstem
- Cerebellothalamic pathways
Spinal cord
Peripheral nervous system
Determining the anatomical origin has important implications for diagnosis and pathophysiology.
Diagnostic Workup
MRI brain was normal.
PET-CT was unrevealing.
CSF studies were normal.
Autoimmune encephalitis antibodies were negative.
Paraneoplastic antibodies were negative.
Inflammatory markers were normal.
No alternative infectious process was identified.
Thus, conventional testing failed to provide an explanation.
Neurophysiology Becomes the Key
EMG demonstrated synchronized rhythmic bursts corresponding to the jerks.
Simultaneous EEG recording showed no epileptiform discharges.
Back averaging revealed no jerk-locked cortical potential.
Somatosensory evoked potentials were not enlarged.
These findings argued strongly against cortical myoclonus.
Teaching Point
Absence of EEG-EMG correlation and lack of giant somatosensory evoked potentials suggest a subcortical origin.
The brainstem is thought to be the most likely source.
This localization fit remarkably well with the associated cerebellar syndrome.
Differential Diagnosis Revisited
Prion disease
Unlikely because:
- Rapid progression was absent.
- MRI was normal.
- Recovery occurred.
Autoimmune encephalitis
Less likely:
- Normal CSF
- Negative antibodies
- No encephalopathy
Drug-induced myoclonus
No offending medications were identified.
Structural lesion
MRI and PET-CT were unrevealing.
Post-infectious immune-mediated syndrome
Supported by:
- Two-week latency after infection.
- Progressive neurological syndrome.
- Lack of alternative causes.
- Dramatic steroid responsiveness.
Final Diagnosis
Post-COVID Myoclonus-Ataxia Syndrome
with electrophysiologic evidence supporting a subcortical (brainstem) origin of the myoclonus.
Management
Because intravenous immunoglobulin was financially prohibitive, treatment consisted of:
- Intravenous methylprednisolone 1 g/day
- Clonazepam
- Levetiracetam
Gradual improvement followed.
Three weeks later, she was discharged.
At two months, she reported approximately 90% recovery and no longer required medication.
Why Did Steroids Work?
The delayed onset following infection suggests a para-infectious or post-infectious immune process rather than direct viral invasion.
Current evidence increasingly supports cytokine-mediated neuroinflammation and autoimmune mechanisms.
This parallels other post-infectious neurological disorders, including:
- Guillain–Barré syndrome
- Acute disseminated encephalomyelitis
- Opsoclonus-myoclonus syndrome
Clinical Pearls
Pearl #1
Myoclonus and ataxia developing 1–3 weeks after COVID-19 should raise suspicion for a post-infectious syndrome.
Pearl #2
Normal MRI and CSF do not exclude an immune-mediated neurological disorder.
Pearl #3
Neurophysiology may be the most important diagnostic study in unexplained myoclonus.
Pearl #4
Absence of EEG correlates points away from cortical myoclonus.
Pearl #5
Prompt immunotherapy is associated with excellent outcomes.
Clinical Pitfalls
Mistaking the jerks for seizures.
Assuming a normal MRI excludes serious neurological disease.
Failing to recognize stimulus sensitivity.
Delaying immunotherapy while awaiting antibody studies.
Attributing symptoms solely to anxiety or functional neurological disorder.
Board-Style Questions
Question 1
A 52-year-old woman develops generalized stimulus-sensitive myoclonus and gait ataxia two weeks after recovering from mild COVID-19. Brain MRI and cerebrospinal fluid studies are unrevealing. Which mechanism is most strongly suggested by the temporal course and clinical presentation?
A. Direct viral invasion of the central nervous system
B. Hypoxic brain injury
C. Post-infectious immune-mediated neuroinflammation
D. Prion disease
E. Drug-induced serotonin syndrome
Answer
C. Post-infectious immune-mediated neuroinflammation
Explanation
The correct answer is C.
The approximately two-week interval between systemic COVID-19 symptoms and the onset of neurological manifestations strongly suggests a post-infectious autoimmune process. Similar delays are seen in Guillain–Barré syndrome and acute disseminated encephalomyelitis. Direct viral invasion would be expected to occur during the acute phase of infection rather than after clinical recovery. The absence of hypoxia, encephalopathy, and exposure to serotonergic medications further argues against the other possibilities. The patient's excellent response to corticosteroids also supports an immune-mediated mechanism.
Question 2
Which electrophysiological finding most strongly argues against cortical myoclonus?
A. Presence of dysarthria
B. Generalized jerking movements
C. Absence of EEG-EMG correlation
D. Action-induced myoclonus
E. Stimulus sensitivity
Answer
C. Absence of EEG-EMG correlation
Explanation
The correct answer is C.
Cortical myoclonus is characterized by electrophysiological evidence of cortical involvement, including EEG correlates, giant somatosensory evoked potentials, and jerk-locked cortical potentials. In this case, simultaneous EEG and EMG recordings failed to demonstrate any correlation, making a cortical origin unlikely. Instead, these findings point toward subcortical or brainstem myoclonus.
Stimulus sensitivity and action-induced jerks can occur in either cortical or subcortical forms and therefore are less specific. Dysarthria simply reflects associated cerebellar involvement and does not localize the myoclonus itself.
Question 3
The coexistence of dysarthria, nystagmus, dysmetria, and wide-based gait localizes primarily to which structure?
A. Basal ganglia
B. Cerebellum
C. Frontal lobe
D. Peripheral nervous system
E. Spinal cord
Answer
B. Cerebellum
Explanation
The correct answer is B.
Dysmetria, impaired rapid alternating movements, gait ataxia, dysarthria, and nystagmus are classic signs of cerebellar dysfunction. Together, these findings localize to the cerebellum and its connections.
Basal ganglia disease typically causes bradykinesia, rigidity, or chorea rather than limb dysmetria and nystagmus. Peripheral nerve and spinal cord disorders do not produce ocular movement abnormalities or cerebellar signs. Recognition of cerebellar involvement is important because the combination of cerebellar dysfunction and generalized myoclonus forms the characteristic myoclonus-ataxia syndrome.
Question 4
Which treatment is most appropriate for suspected post-infectious COVID-19-associated myoclonus-ataxia syndrome?
A. Carbidopa-levodopa
B. Acetazolamide
C. Intravenous methylprednisolone
D. Donepezil
E. Haloperidol
Answer
C. Intravenous methylprednisolone
Explanation
The correct answer is C.
High-dose intravenous corticosteroids represent first-line immunotherapy for many post-infectious neurological disorders. Intravenous immunoglobulin and plasma exchange are alternative therapies when corticosteroids are ineffective or contraindicated.
In this patient, treatment with intravenous methylprednisolone, along with symptomatic therapy using clonazepam and levetiracetam, resulted in dramatic improvement and near-complete recovery. Dopaminergic agents, acetazolamide, acetylcholinesterase inhibitors, and antipsychotics have no established role in treating post-COVID myoclonus-ataxia syndrome.
Question 5
A patient presents with generalized myoclonus, ataxia, and dysarthria two weeks after COVID-19 infection. MRI, PET imaging, and cerebrospinal fluid studies are normal. What is the most important next diagnostic study?
A. Muscle biopsy
B. Temporal artery biopsy
C. Video EEG with electromyography
D. Skin biopsy for small fiber neuropathy
E. Carotid ultrasonography
Answer
C. Video EEG with electromyography
Explanation
The correct answer is C.
When structural imaging and routine laboratory studies are unrevealing, neurophysiological testing becomes essential. Simultaneous EEG and EMG recordings allow clinicians to determine whether the myoclonus originates from the cortex or from subcortical structures.
In this case, the absence of EEG correlates established a subcortical origin and provided important insight into the underlying pathophysiology. Neurophysiology often provides information that conventional MRI cannot and is one of the most valuable diagnostic tools in the evaluation of unexplained myoclonus.
Teaching Pearl
Normal MRI and cerebrospinal fluid studies do not exclude significant neurological disease. In patients with unexplained myoclonus, neurophysiological testing may provide the most important clue to anatomical localization and ultimately guide diagnosis and treatment.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in