Why Latinas Are More at Risk for Cervical Cancer and the Role of the Vaginal Microbiome
Published in Social Sciences, Cancer, and Microbiology

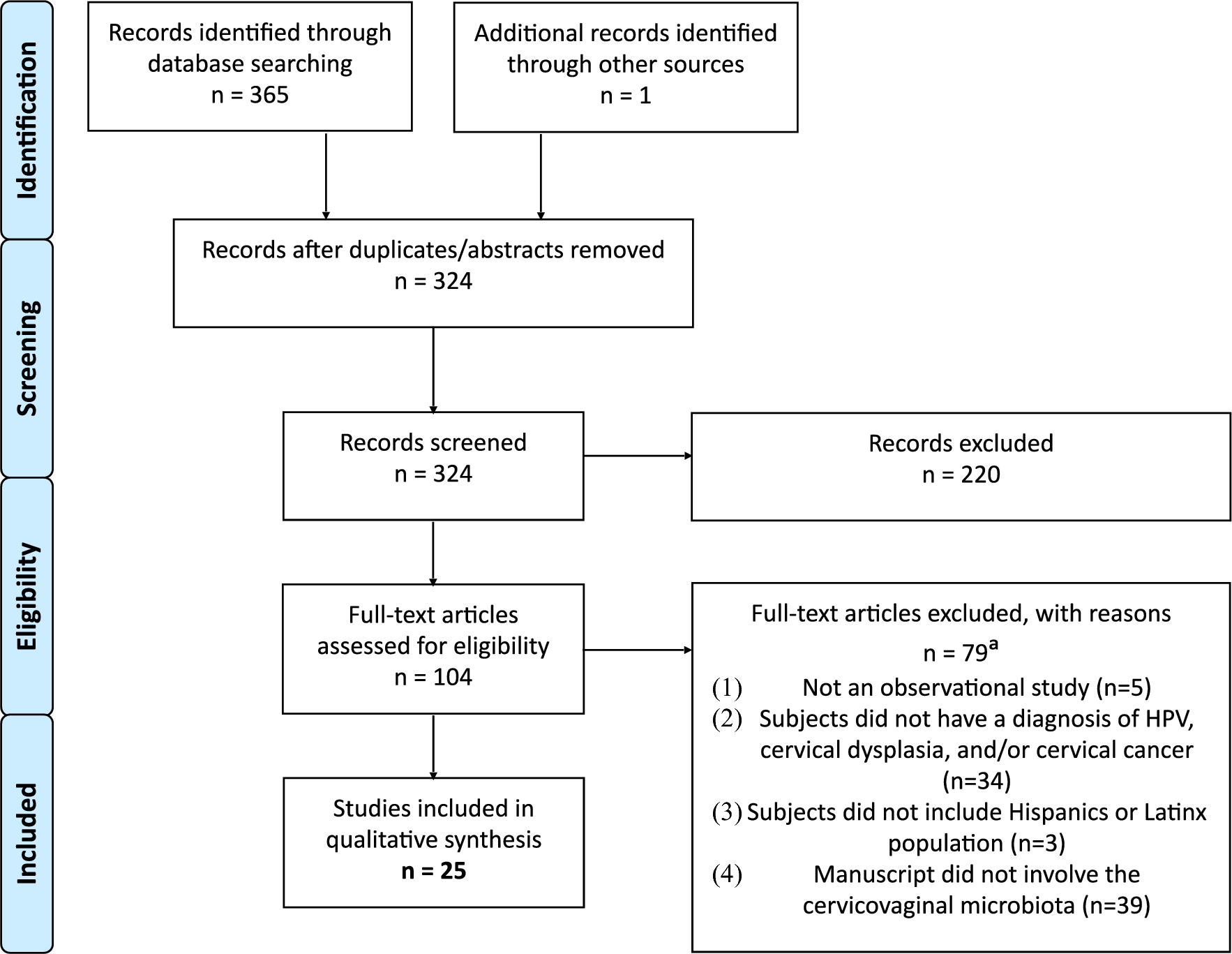


Figure 1. The Vaginal Microbiome, HPV infection, and Cervical Carcinogenesis: A Systematic Review in the Latina Population. Background, Approach, and Key Findings. Created on Canva, by Vianney Mancilla.
How it all began
The impetus for the systematic review began with findings from a cervical cancer cohort led by the Herbst-Kralovetz Lab in Phoenix, Arizona, in 2018 [1]. In a cohort of Arizonan women with equal participation of Hispanic and Non-Hispanic White women, the group identified associations between specific vaginal microbes, Hispanic ethnicity, and cervical carcinogenesis
During the summer of 2022, the Herbst-Kralovetz Lab welcomed a Blaiser/Frontera summer mentee, Vianney Mancilla. The University of Arizona’s Blaiser/Frontera program is designed to prepare undergraduate students historically underrepresented in medicine with the skills and experiences necessary to be competitive medical school applicants. Among these opportunities includes conducting a research project with a renowned faculty mentor at the University of Arizona. What began as an undergraduate summer literature search project that encapsulated Vianney’s passion for health disparities and women’s health and the Herbst-Kralovetz Lab’s interest in investigating cancer risk in Latina study populations, evolved into a systematic review on the topic of her summer research project.
The depletion of health-associated lactobacilli and overgrowth of anaerobes such as Gardnerella, Prevotella, Sneathia, Fannyhessea, and others are associated with bacterial vaginosis (BV). Bacterial vaginosis is linked to numerous adverse gynecologic sequelae and reproductive health outcomes. Notably, women with BV have an increased risk of acquiring sexually transmitted infections, including human papillomavirus (HPV) [2]. Over 90% of HPV infections are cleared, but persistent re-infection of high-risk HPV genotypes can lead to the premalignant precursor, cervical intraepithelial neoplasia (CIN), and ultimately, cervical cancer [3]. Evidence supports the dual role of the cervicovaginal microbiota in HPV clearance through lactobacilli dominance and HPV persistence and cervical cancer development promoted by a dysbiotic shift to BV-associated bacteria, respectively [4].
Latinas have among the highest rates of BV and HPV infection and are 40% more likely to be diagnosed with cervical cancer compared to other racial and ethnic groups [5,6]. This disparity could be exacerbated by systemic barriers that prevent Latinas from receiving access to adequate healthcare services, including HPV vaccination, cervical cancer screenings, and health education [7]. Despite experiencing the highest cervical cancer morbidity and mortality rates, the Latina population continues to be under researched in terms of the vaginal microbiome, HPV, and cervical cancer studies [6]. To identify key vaginal microbes from women more globally, we conducted a systematic review to identify bacteria reported in the VMB of Latinas relating to HPV infection, cervical dysplasia, and cervical cancer, as well as to better understand the role of the microbiome in these disease states across Latin America.
We gathered a team of diverse, inclusive, and transdisciplinary authors dedicated to paving a path to health equity. Our expertise in different areas including pathology, microbiology, epidemiology, and library and information science, allowed for integral conversations on structural racism and factors relating to health disparities while maintaining discussion on race and ethnicity as a non-biological factor. In addition, a number of the investigative team members also identify as Latina or Mexican-American (Chicana), offering a personal and unique perspective on this topic.
What we learned
PubMed, EMBASE, and Scopus databases were searched to include observational studies reporting on the cervicovaginal microbiota in premenopausal Latina women with HPV infection, cervical dysplasia, and cervical cancer. Twenty-five articles were eligible for final inclusion (N = 131,183), and forty-two unique bacteria were reported in the VMB of Latinas across ten countries in North, Central, and South America, and the Caribbean.
In multiple included studies, seven bacteria were consistently enriched across various stages of cervical carcinogenesis in Latinas. Lactobacillus crispatus was associated with health and dysplasia, whereas Lactobacillus iners was associated with health, HPV infection, and dysplasia. Three bacteria, Chlamydia trachomatis, Prevotella amnii, and Prevotella spp. were enriched in the HPV and dysplasia groups. Enrichment of Fusobacterium spp. was detected in Latinas with cervical cancer. Notably, emerging pathogens, Sneathia spp. were enriched across all stages of cervical carcinogenesis and continue to be microbes of interest in this setting.
Additional findings reported an enrichment of L. iners in Latinas, and increased rates of Lactobacillus depletion in Latinas compared to non-Latinas. Our study supports previously reported racial-ethnic differences in VMB composition which reveals an abundance of diverse anaerobes and a depletion of health-associated Lactobacillus species in Black and Hispanic women compared to White and Asian women [8, 9].
Why does this matter?
This study identifies 42 unique bacteria and consistent enrichment of seven bacteria across various stages of cervicovaginal carcinogenesis in Latinas. Longitudinal microbiome studies and larger cohort studies, including Latinas will help determine the role of these bacteria as drivers (influential disease-causing agents), passengers (less influential agents favoring the environment), or a consequence of disease in this population of women [10]. Additionally, varying study designs and a general lack of homogeneity of reported analyses (e.g., few and dissimilar statistical tests, differing variables, etc.) did not meet the basic criteria for unbiased meta-analytic methods. A call for standardization in study methods and analyses across VMB studies can lead to the development of robust conclusions on risk for HPV infection, cervical dysplasia, and cancer outcomes in Latinas. Lastly, advanced public health efforts, including community-based participatory research projects with Latinas, can reduce health disparities in HPV infection and cervical cancer [11].
Overall, this study provides insight to guide future cervicovaginal microbiome research to better inform cervical cancer prevention strategies in Latinas. Intervention through VMB modulation with lactobacilli-based probiotics may improve patient outcomes in this highly susceptible population by promoting HPV clearance and regression of disease [12].

To read more about our systematic review, read the full article in Journal of Epidemiology and Global Health: The Vaginal Microbiota, Human Papillomavirus Infection, and Cervical Carcinogenesis: A Systematic Review in the Latina Population
References
- Łaniewski P, Barnes D, Goulder A, et al. Linking cervicovaginal immune signatures, HPV and microbiota composition in cervical carcinogenesis in non-Hispanic and Hispanic women. Sci Rep. 2018;8(1):7593. Published 2018 May 15. doi:10.1038/s41598-018-25879-7
- Łaniewski P, Herbst-Kralovetz MM. Bacterial vaginosis and health-associated bacteria modulate the immunometabolic landscape in 3D model of human cervix. NPJ Biofilms Microbiomes. 2021;7(1):88. Published 2021 Dec 13. doi:10.1038/s41522-021-00259-8
- Plummer M, Schiffman M, Castle PE, Maucort-Boulch D, Wheeler CM, ALTS Group. A 2-year prospective study of human papillomavirus persistence among women with a cytological diagnosis of atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesion. J Infect Dis. 2007;195(11):1582–9. https://doi.org/10.1086/516784.
- Ntuli L, Mtshali A, Mzobe G, Liebenberg LJ, Ngcapu S. Role of Immunity and Vaginal Microbiome in Clearance and Persistence of Human Papillomavirus Infection. Front Cell Infect Microbiol. 2022;12:927131. Published 2022 Jul 7. doi:10.3389/fcimb.2022.927131
- Peebles K, Velloza J, Balkus JE, McClelland RS, Barnabas RV. High global burden and costs of bacterial vaginosis: a systematic review and meta-analysis. Sex Transm Dis. 2019;46(5):304–11. https://doi.org/10.1097/OLQ.0000000000000972.
- Ortiz AP, Soto-Salgado M, Calo WA, et al. Elimination of cervical cancer in U.S. Hispanic populations: Puerto Rico as a case study. Prevent Med. 2021;144:106336. https://doi.org/10.1016/j.ypmed.2020.106336.
- Almonte M, Albero G, Molano M, Carcamo C, García PJ, Pérez G. Risk factors for human papillomavirus exposure and co-factors for cervical cancer in Latin America and the Caribbean. Vaccine. 2008;26:L16–36. https://doi.org/10.1016/j.vaccine.2008.06.008.
- Ravel J, Gajer P, Abdo Z, et al. Vaginal microbiome of reproductive-age women. Proc Natl Acad Sci. 2011;108(supplement_1):4680–7. https://doi.org/10.1073/pnas.1002611107.
- MacIntyre DA, Chandiramani M, Lee YS, et al. The vaginal microbiome during pregnancy and the postpartum period in a European population. Sci Rep. 2015;5(1):8988. https://doi.org/10.1038/srep08988.
- Łaniewski P, Ilhan ZE, Herbst-Kralovetz MM. The microbiome and gynaecological cancer development, prevention and therapy. Nat Rev Urol. 2020;17(4):232. https://doi.org/10.1038/s41585-020-0286-z.
- Barnack-Tavlaris JL, Garcini L, Sanchez O, Hernandez I, Navarro AM. Focus group discussions in community-based participatory research to inform the development of a human papillomavirus (HPV) Educational Intervention for Latinas in San Diego. J Cancer Educ. 2013. https://doi.org/10.1007/s13187-013-0516-0517.
- Mei Z, Li D. The role of probiotics in vaginal health. Front Cell Infect Microbiol. 2022;12:963868. Published 2022 Jul 28. doi:10.3389/fcimb.2022.963868
Follow the Topic
-
Journal of Epidemiology and Global Health
The journal aims to impact global epidemiology and international health with articles focused on innovative scholarship and strategies to advance global health policy.

Related Collections
With Collections, you can get published faster and increase your visibility.
Climate and Environmental Change as Drivers of Infectious Disease: A Planetary Health Perspective
Human health is increasingly shaped by the interconnected pressures of climate change, environmental degradation, and socio‑ecological disruption. These planetary‑scale changes influence not only the epidemiology of infectious diseases, but also the public health systems, social structures, and community capacities that determine exposure, vulnerability, and resilience. This Collection adopts a planetary health perspective to explore how climate variability, ecosystem disruption, and human–environment interactions affect infectious disease risks and the public health responses needed to address them.
We welcome research that examines how shifts in temperature, precipitation, humidity, extreme weather events, land‑use change, biodiversity loss, and urbanization influence pathogen ecology, transmission pathways, and population vulnerability. Beyond epidemiological patterns, the Collection seeks contributions that address preparedness, surveillance, health system resilience, risk communication, governance, and cross‑sectoral interventions aimed at mitigating and adapting to climate‑related infectious disease threats.
Studies leveraging epidemiological datasets, climate and environmental records, spatial mapping, and predictive modeling are encouraged, as are qualitative, policy‑focused, and implementation‑oriented works that illuminate barriers and opportunities within public health systems. Particular attention is given to inequities in exposure and resilience, the needs of high‑risk populations, and the role of community‑level and institutional adaptation strategies.
By integrating epidemiology, environmental science, and public health practice, this Collection aims to advance understanding of climate–disease interactions, strengthen early warning and response systems, and inform adaptive strategies that protect and promote planetary health in a rapidly changing world. Topics of interest include but are not limited to:
- Climate‑sensitive infectious diseases and changing transmission patterns
- Impacts of extreme weather events and environmental disruption on disease risk
- Public health preparedness, surveillance, and early warning systems
- Health system resilience and climate adaptation strategies
- Socio‑ecological vulnerability, inequities, and community resilience
- Land‑use change, biodiversity loss, and zoonotic spillover
- Modeling climate, environmental, and disease interactions
- Governance, policy, and multisectoral responses to planetary health threats
- One Health and Planetary Health approaches to infectious disease prevention
This Collection supports and amplifies research related to SDG 13, Climate actions.
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Mar 31, 2027
Public Health Professionals’ Education
Strengthening the education and continuous professional development of public health professionals is fundamental to achieving resilient, equitable, and responsive health systems. Recent global experiences including pandemics, protracted humanitarian crises, climate-related health risks, rapid urbanization, and technological transformation have highlighted both the critical role of the public health workforce and persistent gaps in training relevance, scale, quality, and sustainability. In many settings, educational models remain insufficiently aligned with real-world system needs, emerging competencies, and evolving career pathways.
While there is growing innovation in public health education, evidence and lessons learned are dispersed across disciplines and regions. A focused supplement in the Journal of Epidemiology and Global Health will provide a timely scholarly platform to consolidate high-quality research and practice-based insights.
The proposed Collection aims to advance knowledge in the education of public health professionals by:
Showcasing empirical evidence and innovative models for public health education and training
Examining how educational approaches align with health system priorities and workforce needs
Informing policy, institutional strategies, and investment in public health workforce development
Promoting equity, quality, and sustainability in public health education globally.
Scope and Thematic Areas
The supplement will invite original research articles, systematic or scoping reviews, and rigorously documented practice-based papers across the following thematic areas:
Competency-Based Public Health Education
- Core and advanced competency frameworks
- Alignment of curricula with population health needs and system priorities
Field-Based and Applied Learning Models
- Field Epidemiology Training Programs (FETPs) and similar applied training models
- Experiential learning, service-based education, and community engagement
Interprofessional and Multisectoral Education
- Collaborative training across health, social, environmental, and humanitarian sectors
- Preparing public health professionals for whole-of-government and whole-of-society approaches
Digital, Blended, and Distance Learning Innovations
- Online and hybrid training models
- Use of digital platforms, simulation, and emerging technologies in education
Education for Health Emergencies and Fragile Settings
- Workforce training for outbreak preparedness, humanitarian response, and conflict settings
- Adaptive education models in fragile and resource-constrained contexts
Equity, Ethics, and Inclusion in Public Health Training
- Gender, geographic, and socioeconomic equity in access to education
- Ethical dimensions of training, mentorship, and professional advancement
Leadership, Management, and Systems Thinking
- Training for public health leadership, governance, and policy engagement
- Building managerial and strategic competencies for system-level impact
Mentorship, Supervision, and Career Pathways
- Structured mentorship and supervision models
- Transition from training to practice and career progression
Monitoring, Evaluation, and Impact of Public Health Education
- Methods for assessing educational outcomes and workforce impact
- Long-term sustainability and return on investment of training programs
Partnerships, Financing, and Institutionalization
- Academic–government–partner collaborations
- Financing models and institutional integration of training programs
All submissions in this collection undergo the journal’s standard peer review process. Similarly, all manuscripts authored by a Guest Editor(s) will be handled by the Editor-in-Chief. As an open access publication, this journal levies an article processing fee (details here). We recognize that many key stakeholders may not have access to such resources and are committed to supporting participation in this issue wherever resources are a barrier. For more information about what support may be available, please visit OA funding and support, or email OAfundingpolicy@springernature.com or the Editor-in-Chief.
Publishing Model: Open Access
Deadline: Dec 17, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in