MMPs and TIMPs in delirium
Published in Neuroscience, Cell & Molecular Biology, and Immunology

If you have ever visited a loved one in the hospital during severe illness, for example after a surgical hip fracture repair, you might have witnessed sudden disturbances in attention, confusion or even frightening hallucinations. In other words, you might have witnessed an episode of delirium, a common complication in acute illness. This syndrome is especially common among older persons and those suffering from cognitive impairment or dementia. Delirium is distressing to experience and witness. A person with delirium might become scared and confused, and suddenly believe that the treating doctors or nurses are aliens or ghosts out to hurt them.
While distressing in its own right, delirium is also connected to increased morbidity and future dementia risk. Therefore, it is important to prevent, recognise and treat delirium – but the syndrome is underdiagnosed and poorly understood. Moreover, there are several key challenges that hamper progress in the scientific study of delirium:
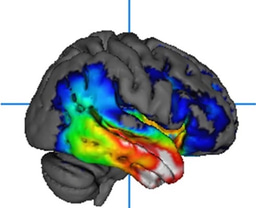
- Many of the techniques commonly applied to study the brain, such as neuroimaging are often not possible to perform during a delirium episode – just imagine being confused about where you are and what is happening, and then being asked to be lie very still inside a loud machine for several minutes!
- Delirium is triggered by an acute trauma, such as infection with sepsis or surgery. This trauma could also affect the brain, making it challenging to figure out if observations are caused by delirium or by the trigger.
- Cognitive impairment and dementia increase the risk of delirium significantly. Dementia can have many of the same symptoms as delirium and is often caused by underlying disease in the brain – it can therefore be a challenge to separate the effects of dementia and the effects of delirium, both in terms of symptoms and in terms of changes in the brain.
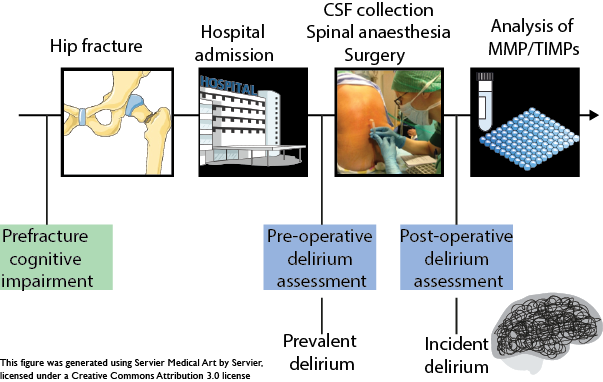
To face the first challenge, we study proteins in the cerebrospinal fluid (CSF). Inside your body, the CSF is produced in the brain and fills the cavities surrounding the brain and spinal cord. This fluid provides a unique window into the brain, as changes in the proteins and metabolites in the CSF can give us information about the status of the brain. We studied the CSF from 280 hip fracture patients who were undergoing surgery in spinal anaesthesia. When patients are operated in spinal anaesthesia, CSF can be collected without any further risk to the patient. Moreover, hip fracture patients have a high risk of developing delirium and indeed, half of the patients in our cohort did.
To face the second challenge and third challenge, disentangling the effects of acute trauma and dementia, we included two other patient groups who did not experience acute trauma for comparison. One group included 107 cognitively unimpaired older persons and one group included 111 patients with dementia due to Alzheimer’s disease.
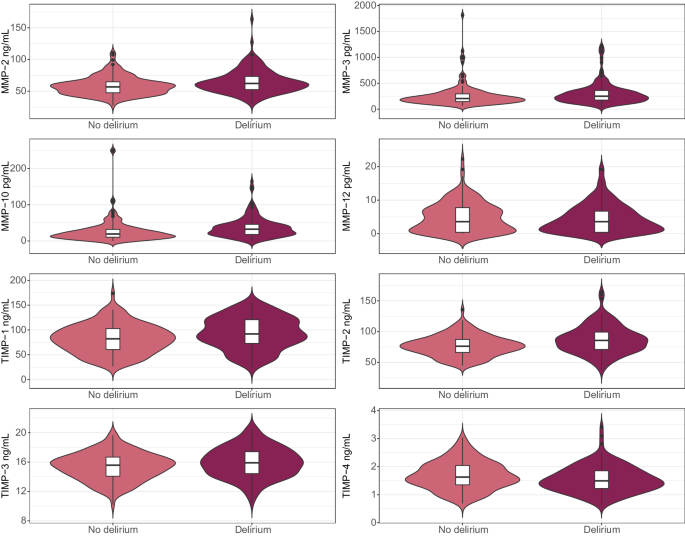
Inflammation in the brain – neuroinflammation – is thought to be connected to the development of delirium. Therefore, we studied a family of proteins with important roles in neuroinflammation: matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs). This is the first time these proteins have been studied in the CSF in patients with delirium. We found that:
- Most of the measured proteins differed between the hip fracture patients and both control groups, suggesting that acute trauma such as hip fracture could influence these proteins.
- Several of the proteins differed in the hip fracture patients with delirium compared to those who did not have delirium. But most of the patients with delirium also had dementia. Most of the differences between the patients with delirium and the patients without delirium were likely due to dementia, as we found similar changes in protein levels in the patients with Alzheimer’s disease dementia.
- One marker was associated with delirium, even when accounting for the influence of age, sex and dementia. This marker, TIMP-4, could be directly linked to changes in the brain that cause delirium. We speculate that low levels of this protein could reflect an insufficient response to acute damage and predispose patients to delirium.
To conclude, delirium is common, distressing and associated with increased risk of serious health outcomes such as dementia and death. Unfortunately, delirium is at the same time underdiagnosed and understudied. It is challenging to study what happens in the brain during delirium, and to separate the effects of delirium from predisposing factors such as acute trauma and dementia. In our study, we studied proteins in the CSF to get insight into brain processes during delirium; we further compared levels of the proteins with two control groups without acute trauma, one without and one with dementia. Our study design illustrated that while several proteins were associated with delirium, most could also be linked to acute trauma or pre-existing dementia. However, low levels of the protein TIMP-4 are linked to delirium and its role in the development of this syndrome should be explored further.
Follow the Topic
-
Communications Medicine

A selective open access journal from Nature Portfolio publishing high-quality research, reviews and commentary across all clinical, translational, and public health research fields.
Ask the Editor - Immunology, Pathogenesis, Inflammation and Innate Immunity
Got a question for the editor about the complement system in health and disease? Ask it here!
Continue reading announcementRelated Collections
With Collections, you can get published faster and increase your visibility.
Healthy Aging
Publishing Model: Open Access
Deadline: Jun 01, 2026
Public health and health governance in China
Publishing Model: Open Access
Deadline: Apr 30, 2026

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in