Modern polygenetic scores resonate with the historical landmark distinction between bipolar disorder and schizophrenia
Published in Behavioural Sciences & Psychology
More than a century ago, Emil Kraepelin laid the foundation for distinguishing between manic-depressive psychosis and dementia praecox, now recognized as bipolar disorder (BD) and schizophrenia, respectively. The hallmark of BD consists of disruptive episodes of mania and depression between which patients typically recover and regain function. Psychotic symptoms may occur during mood episodes but are absent during euthymic periods. This course of illness contrasts the prototypical form of schizophrenia that follows a chronic, deteriorating course. Although psychotic symptoms may wax and wane in schizophrenia, negative symptoms persist and full recovery is rare. However, the actual clinical presentation and natural course of BD vary considerably among individuals. While many patients achieve complete inter-episode remission and regain full function between mood episodes, a significant portion experiences lingering mood symptoms or cognitive impairment that hinder full functional recovery.
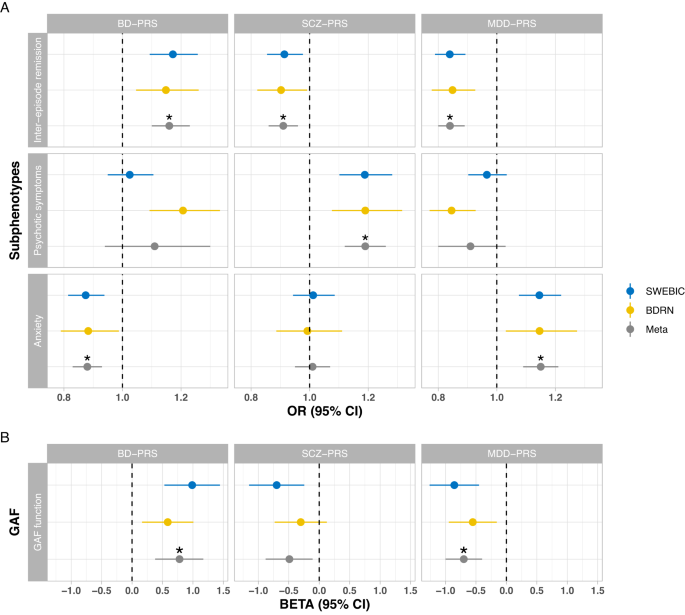
In an effort to bridge the gap between traditional categorical distinctions in psychiatric diagnostic systems and the evolving understanding of disorders as dimensional entities with polygenic underpinnings, we conducted a comprehensive investigation into the genetic susceptibilities of BD, schizophrenia, and major depressive disorder (MDD) in relation to key BD subphenotypes. We calculated polygenic risk scores (PRS) from two large BD cohorts in Sweden and the UK, and examined their associations with inter-episode remission, global functioning, symptom burden, psychotic features during mood episodes, and the presence of comorbid anxiety disorders.
Intriguingly, our findings revealed that complete inter-episode remission was associated with higher BD-PRS and lower SCZ-PRS, mirroring the prototypical episodic course of illness of BD and the chronic course of schizophrenia. Further, we found that higher global functioning was associated with higher BD-PRS and lower SCZ-PRS. This again aligns with the Kraepelinian concept of schizophrenia as a disorder characterized by a chronic, deteriorating course with persistent impairment, in contrast to individuals with BD who tend to be symptom-free when recovered from mood episodes.
Assuming a higher PRS of a certain psychiatric disorder in cases with a positive family history, we also examined BD subphenotypes in a familial coaggregation design using Swedish national registries. This involved comparing BD index individuals who had a relative with BD with those whose relative had schizophrenia. Consistent with the polygenic score analyses, BD cases with a family history of schizophrenia had lower global functioning compared with those with a family history of BD. Last, we found that higher MDD-PRS was associated with reduced likelihood of inter-episode remission, lower psychosocial function, and a higher rate of comorbid anxiety disorders. Again, these associations were supported by the familial co-aggregation analyses.
Even though schizophrenia and MDD are the two psychiatric disorders with the highest genetic correlations with BD, there hence seems to be a unique BD genetic component not shared with the two other psychiatric disorders. Whereas PRS derived from schizophrenia and MDD genome-wide association studies partly index a general liability for chronic psychopathology severity, higher genetic loading of BD was associated with higher psychosocial functioning. The latter observation might appear counterintuitive, but it is important to note that psychosocial functioning was assessed in an outpatient setting during which patients are more likely to be recovered with fewer symptoms. Higher BD-PRS is thus associated with better functioning and fewer symptoms when BD patients are not acutely ill. Indeed, higher BD-PRS has been reported to confer benefits in other domains, for example creativity and educational attainment. Notably, this does not imply that higher BD-PRS would be associated with less severe (or less frequent) mood episodes.
Taken together, these modern polygenetic and epidemiological analyses reflect the historical distinction between recurrent manic-depressive insanity and progressive dementia praecox as outlined by Emil Kraepelin. Our findings help explain how genetic factors contribute to the heterogeneous presentations of BD, enhancing our understanding of how polygenic vulnerabilities underpin its multifaceted manifestation.
Follow the Topic
-
Molecular Psychiatry

This journal publishes work aimed at elucidating biological mechanisms underlying psychiatric disorders and their treatment, with emphasis on studies at the interface of pre-clinical and clinical research.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in