Prognostic relevance of the neurological symptom burden in brain metastases from breast cancer
Published in Cancer and General & Internal Medicine
Brain metastases (BM) are a common and serious complication of breast cancer (BC). In recent years, regular brain screenings in cancers that frequently spread to the brain have led to earlier detection, often before symptoms appear. This has raised the question of whether treatment should be adjusted based on the presence or absence of symptoms. Research on lung cancer and melanoma has shown that patients with symptom-free BM tend to live longer than those with symptomatic BM. However, until now, no studies have explored how neurological symptoms affect prognosis in patients with BM from BC.
Therefore, we aimed to explore the frequency of neurological symptoms at diagnosis of BM and evaluate its influence on the prognostic landscape in a unique real-world cohort of patients BC diagnosed between 1992-2020 at the Medical University of Vienna as the foundation for future clinical trial planning and treatment decision-making.
Presence of neurological symptoms in patients with brain metasetases from breast cancer over the last three decades
Clinical examination and history regarding neurological symptom burden were performed routinely at diagnosis of BM and documented in the patient’s record. 716 patients with BM from BC and information on neurological symptoms at diagnosis of BM were included in the study.
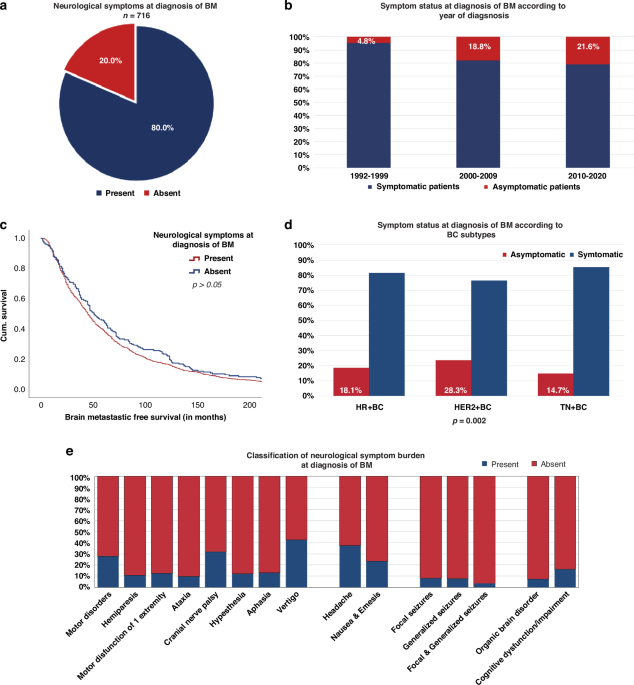
80% (573/716) of the patients presented with neurological symptoms at the time of BM diagnosis: Focal deficits were the most commonly documented neurological symptoms at the time of BM diagnosis (88.0%; 504/573), followed by signs of increased intracranial pressure (48.0%; 275/573), neuropsychological symptoms (31.9%; 183/573) and epileptic seizures (15.7%; 90/573). Patients were classified as asymptomatic if they had no current neurological symptoms and had not experienced any prior neurological symptoms related to the present BM.
Significant correlation of BC receptor status and neurological symptom burden
If information regarding histopathological subtypes by immunohistochemical analysis and ERBB2 amplification was accessible, BC was further classified into hormone receptor-positive; HER2 (human epidermal growth factor receptor 2)-negative breast cancer (HR+BC), HER2 overexpressing breast cancer (HER2+BC), and triple-negative breast cancer (TN-BC). In 653/716 (91.2%) patients, information on the receptor status was available including 260/653 (39.8%) patients with HR+BC, 230/653 (35.2%) with HER2+BC and 163/653 (25.0%) with TN-BC.
Patients with HER2+BC were more frequently diagnosed with asymptomatic BM during staging procedures (65/230; 28.3%), compared to HR+BC (47/260; 18.1%) and TN-BC (24/163; 14.7%). Notably, a numerical increase of asymptomatic patients at the time of BM diagnosis was observed over the last three decades (1992-1999: 4.8% versus 2010-2020: 21.6%; p= 0.135)- irrespective of the underlying BC subtype.
Clinical charactersitics and treatment strategies associated with neurological symptoms
Patients with BM as the only metastatic site had a significantly higher rate of symptomatic disease compared to patients with known extracranial metastasis (p=0.019). This effect was most pronounced in HER2+BC, as 83.7% (41/49) of patients with absent extracranial metastases showed neurological symptoms at diagnosis of BM compared to 68.5% (124/181) of patients with concurrent BM and extracranial disease (p=0.036). This finding indicates that HER2+ BC patients, as a specific high risk group for BM, could benefit from screening in early stages in absence of extracranial disease.
Radiotherapy such as whole brain radiation therapy (WBRT) and focal radiotherapy presented as the predominant therapeutic modality following the diagnosis of BM in BC patients across the decades. However, we observed noteworthy variations in initial treatment strategies upon the symptomatology and BC subtype:
Specifically, among symptomatic patients with HR+BC, WBRT was the predominant choice (50.2%; 107/213), surpassing focal radiotherapy alone (15.5%; 33/213; p<0.001). 14.6% (31/213) of HR+BC patients with neurological symptoms received combinational approaches after diagnosis of BM: 18/31 (58.1%) underwent WBRT along with focal radiotherapy, while 13/31 patients (41.9%) received additional radiation therapy after neurosurgery at the time of BM diagnosis. In asymptomatic patients, regardless of the underlying BC subtype, SRS consistently emerged as the most frequently employed treatment modality over the decades. Moreover, a discernible upward trend in the utilization of systemic therapy as an initial treatment approach after diagnosis of BM was noted in asymptomatic patients across different decades (1992-1999: 0% vs. 2010-2020: 5.6%).
Correlation of neurological symptoms with survival prognosis
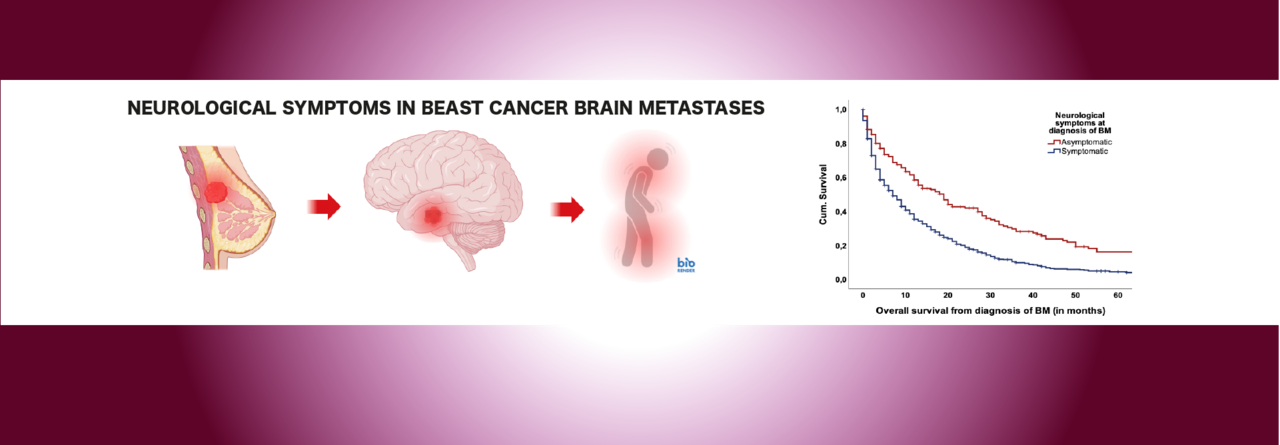
Patients without neurological symptoms at baseline had a significantly prolonged median OS from diagnosis of BM compared to symptomatic patients (20 vs. 9 months, p<0.001). This observed effect persisted consistently across all BC subtypes (HR+BC 29 vs. 9 months; HER2+BC 24 vs. 12 months; TN 12 vs. 6 months; p<0.05) and throughout the three decades (1992-1999: 14 vs. 9 months; 2000-2009: 19 vs. 8 months; 2010-2020: 27 vs. 9 months; p<0.05).
Interestingly, patients with neuropsychological symptoms presented a significantly shorter median OS compared to patients with other neurological symptoms (12 vs. 5 months; p<0.001).
To assess the prognostic independence of neurological symptoms in relation to other prognostic factors, we incorporated parameters such as Breast-GPA, the size of BM at diagnosis, treatment strategies and neurological symptoms into a multivariate model. In this analysis, the presence of neurological symptoms, the treatment approach after BM diagnosis and the Breast-GPA remained independently associated with prognosis.
SUMMARY
This is the first study that includes a detailed characterization of the neurological symptom burden at diagnosis of BM across all subtypes of BC. More importantly, our study identified the presence of neurological symptoms at diagnosis of BM as an independent and strong prognostic factor in a large, distinctive real-world cohort of patients with brain metastatic BC. The outcomes underscore the critical need for subsequent prospective trials to thoroughly examine the integration of neurological symptom burden into prognostic assessments for individuals with BM originating from BC.
Follow the Topic
-
British Journal of Cancer

This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in