Providing quality of care feedback using Bayesian Machine Learning in Urology
Published in Social Sciences, General & Internal Medicine, and Statistics
We developed a new model for facilitating feedback to clinicians using large administrative datasets in urology. The model, known as Variational Inference for Risk Adjustment of General Outcome Indicators (VIRGO), is a high dimensional explainable Bayesian inference model that facilitates quality improvement feedback to be provided to clinicians.
We chose urology as it currently lacks quality improvement indicators. The model developed uses Bayesian variational inference to provide the expected outcomes of a patient based on diagnosis, procedures and comorbidities to provide clear feedback to healthcare professionals.
Our model facilitates decision-making by:
- Having state-of-the-art individualised prediction on length of stay and hospital-acquired complications.
- Allowing hospital administrators and clinicians to highlight cases of interest (outliers) who have unexpectedly long lengths of stay or unexpectedly large counts of hospital-acquired complications.
- Allow for counterfactual analysis, or in other words, allowing for clinicians to ask based on a particular case study, what is the expected outcome if the patient had not developed complications or have diabetes or other comorbidities. Clinicians can remove or add hypothetical variables to understand which particular variable affects the outcome the most.
- The model provides clear explanations of how it derives the prediction of the outcome. With variable weights contributing heavily to the outcome being presented to clinicians for further examination.
As shown in this figure, the model can accurately predict the length of stay and provide not only the expected length of stay, but can an interpretable credible interval, which can be interpreted as "Based on the patient's condition, there is a 99% probability that the length of stay of the patient is predicted to be 0 - 19 days (Figure 1a).
Furthermore, as shown in Figure 1b, healthcare professionals can then ask questions such as "What would happen if the patient did not have surgical complications, and did not require blood transfusion.", as we can see, the prediction range shrinks from 0 - 19 days to 0 - 12 days.
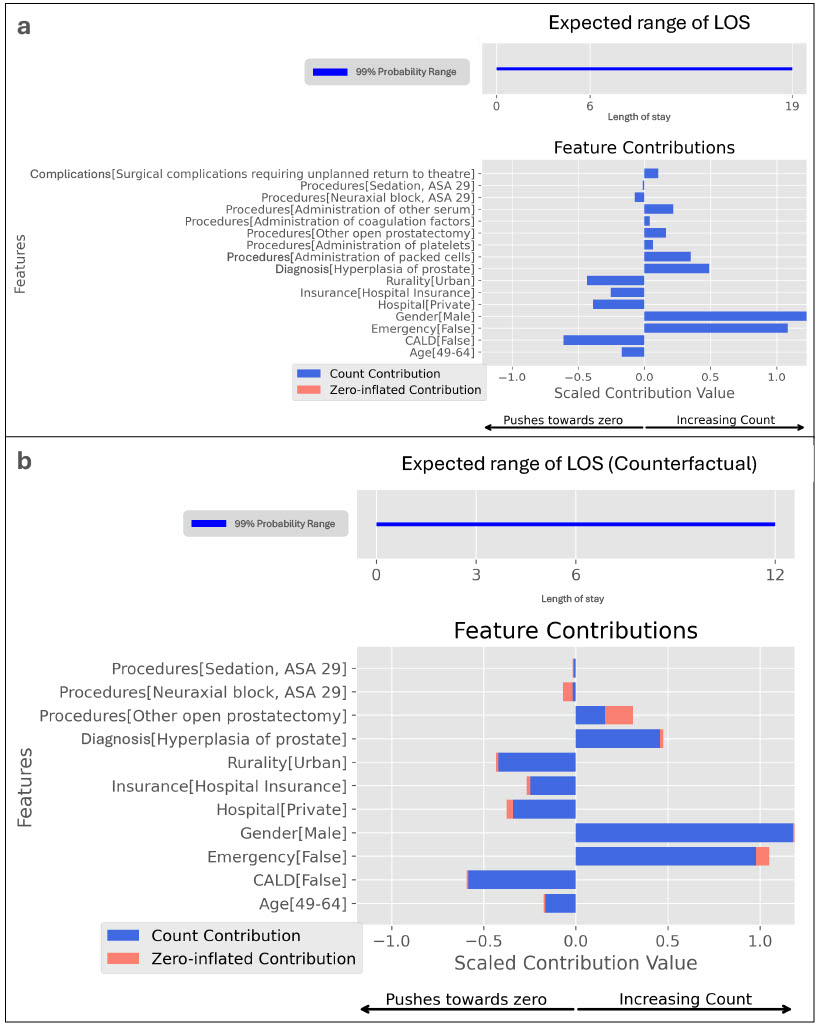
Figure 1: Providing feedback to healthcare professionals via counterfactual analysis. Counterfactual analysis of a patient with surgical complications developed during open prostatectomy for prostate hyperplasia. Figure 1a: Shows the expected range of LOS and the count and zero-inflated parameters that contribute to the overall prediction, given the complications and blood transfusions, the expected LOS within a 99% probability range is predicted to be 0 – 19 days. The feature contribution plot shows that the parameters affecting the overall prediction are mostly count parameters. Figure 1b: Shows the counterfactual analysis of the patient, predicting that the expected range of LOS if the patient did not have complications and blood transfusions. The expected LOS within 99% probability decreases to 0 – 12 days. The feature contribution plot has now changed, with zero-inflated parameters (highlighted in orange) now marginally contributing to the overall prediction.
This represents a step forward in providing good feedback for specialities and areas in which quality improvement is sordidly needed, but lacks the resources to collect data required to generate gold-standard quality indicators (KPI), as the model simply uses the minimally collected electronic health data which is collected by every hospital in Australia.
In the future, we seek to create a unified model that not only works for urology but the entire healthcare system as a whole.
Follow the Topic
-
npj Digital Medicine

An online open-access journal dedicated to publishing research in all aspects of digital medicine, including the clinical application and implementation of digital and mobile technologies, virtual healthcare, and novel applications of artificial intelligence and informatics.
Related Collections
With Collections, you can get published faster and increase your visibility.
Evaluating the Real-World Clinical Performance of AI
Publishing Model: Open Access
Deadline: Jun 03, 2026
Impact of Agentic AI on Care Delivery
Publishing Model: Open Access
Deadline: Jul 12, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in