Quantification of T cell clonality in human T cell leukaemia virus type-1 carriers can detect the development of adult T cell leukaemia early
Published in Cancer

We are a research group comprising of scientists and clinicians, closely affiliated with the National Centre for Human Retrovirology, where we provide lifelong care and specialised diagnostics for people living with the retrovirus Human T cell Leukaemia Virus type-1 (HTLV-1). Here, we see the consequences of HTLV-1 infection daily, from the molecular level to the devastating impact on quality of life.
Five percent of those infected with HTLV-1 will develop a malignancy of CD4+ T lymphocytes called adult T cell leukaemia/lymphoma (ATL). Despite our best efforts to treat the disease, the prognosis is dismal and those that present with the most aggressive subtypes survive for less than a year. In this study, our objective was to identify HTLV-1 carriers at the highest risk of ATL, to improve their care and optimise their outcome [1].
HTLV-1 infects and immortalises CD4+ T cells by inserting a copy of the viral genome into the host cell DNA and establishing infected T cell clones. In ATL, after many years, a single T cell clone becomes dominant [2], due to progressive accumulation of mutations that enhance T cell fitness within that clone. As we knew that driver mutations in ATL can appear many years before disease presentation [3], we hypothesised that changes in T cell clonality would also be apparent long before the carrier becomes unwell.
To quantify differences in T cell clonality between individuals we took advantage of the fact that T cell clones each express a common unique T cell receptor (TCR) which is assembled in a modular fashion from TCR gene subunits. We used a panel of antibodies specific for TCRVbeta subunits to count the number of HTLV-1 infected CCR4+CD26- T cells expressing each of 24 TCRVbeta subunit families circulating in the blood, and thus calculated an 'oligoclonality' score of HTLV-1 infected T cells for each individual.
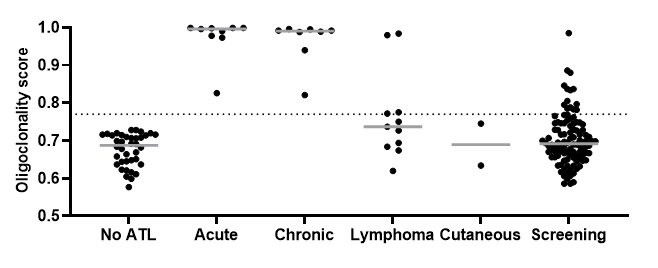
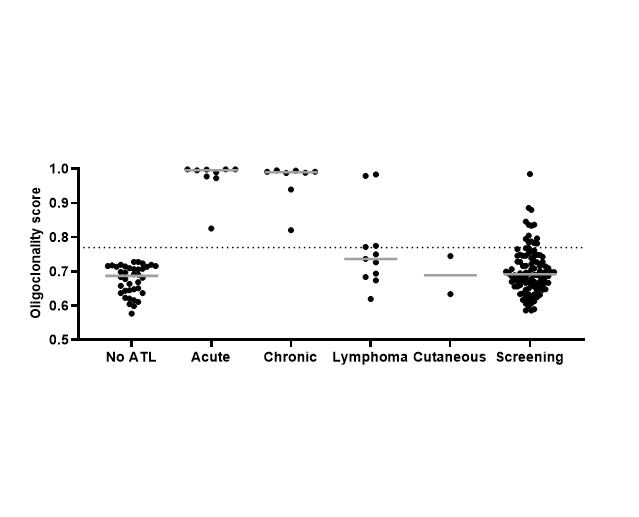
Fig.1 Oligoclonality scores of HTLV-1 infected T cells circulating in the blood
Thanks to the high level of participation of our patients in research, we were able to test blood samples from patients with ATL and stored blood samples of HTLV-1 carriers who we knew had not developed any signs of ATL in the subsequent 10 years, allowing us to determine the range of T cell clonality in healthy carriage of HTLV-1 and ATL.
When we used our protocol to screen 106 patients attending our clinic, we found that almost 20% of HTLV-1 carriers who had a high burden of HTLV-1 infected cells had ATL-like clones circulating in their blood. We followed all of the patients we screened for a total of 129 patient-years. In this period, two patients in whom we observed ATL-like clones were diagnosed with ATL, whereas none of the high burden carriers who did not have an ATL-like clone transformed.
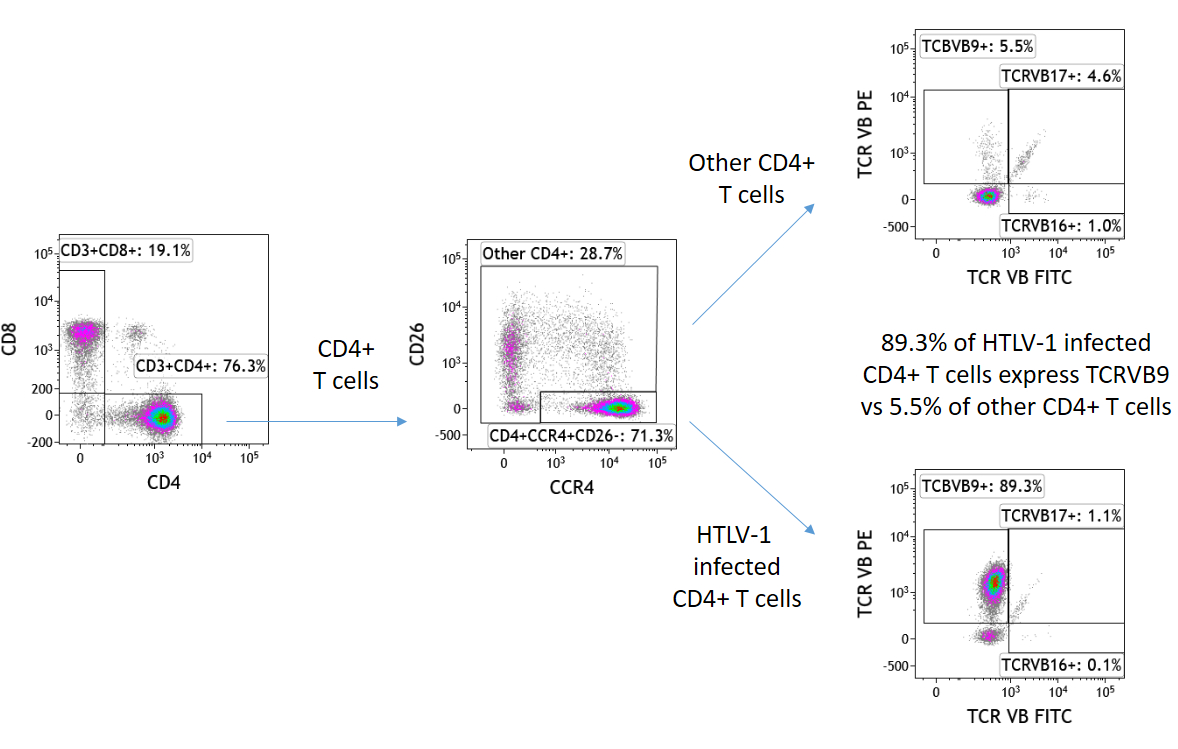
Fig.2 Example flow cytometric staining for TCRVbeta subunits showing an ATL-like clone expressing TCRVbeta9
This observation carries the potential to fundamentally change the clinical management of people at high risk of ATL by supporting strategies to pre-emptively treat high-risk individuals who are in the process of transforming, and is likely to inform public health communicable disease screening and monitoring strategies. Many HTLV-1 carriers come from low and middle income countries, or are diaspora populations who often suffer healthcare marginalisation, and HTLV-1 has historically been somewhat side-lined despite its potential for understanding the interactions between viruses and cancer [5].
The current global pandemic has naturally affected our research: clinics becoming virtual, lab space requiring social distancing, and clinicians being redeployed mid-research. As we work towards ‘the new normal’, we continue to follow this cohort of high-risk patients, and soon we will start to test early intervention strategies to deplete ATL-like clones in high-risk carriers, with the ultimate goal of preventing ATL.
References
- Wolf SN, Haddow J, Greiller C et al. Quantification of T cell clonality in human T cell leukaemia virus type-1 carriers can detect the development of adult T cell leukaemia early. Blood Cancer J 2021, Mar 26;11(3):66.
- Cook LB, Melamed A, Niederer H et al. The role of HTLV-1 clonality, proviral structure, and genomic integration site in adult T-cell leukemia/lymphoma. Blood 2014; 123: 3925-3931.
- Rowan AG, Dillon R, Witkover A et al. Evolution of retrovirus-infected premalignant T-cell clones prior to adult T-cell leukemia/lymphoma diagnosis. Blood 2020; 135: 2023-2032.
- Rowan AG, Witkover A, Melamed A et al. T Cell Receptor Vbeta Staining Identifies the Malignant Clone in Adult T cell Leukemia and Reveals Killing of Leukemia Cells by Autologous CD8+ T cells. PLoS Pathog 2016; 12: e1006030.
- World Health Organisation. Human T-lymphotropic virus type 1: technical report https://apps.who.int/iris/handle/10665/339773
Follow the Topic
-
Blood Cancer Journal
This journal seeks to publish articles of the highest quality related to hematologic malignancies and related disorders.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in