Racial and ethnic disparities in ovarian cancer survival
Published in Cancer and General & Internal Medicine
As an ovarian cancer researcher for nearly ten years, I have been lucky to have been involved in many international consortium studies that bring together large datasets to address different questions. The Ovarian Cancer Association Consortium (OCAC) and Ovarian Tumor Tissue Analysis Consortium are examples of global partnerships to examine factors associated with ovarian cancer risk and survival.
The OCAC have published countless studies, and the next important step was to examine whether there are differences in survival outcomes for patients from different racial and ethnic groups. Towards this goal, we analysed information from nearly 15,000 women diagnosed with epithelial ovarian cancer, spanning Australia, North America, and Europe. This scale of collaboration allowed us to examine something that smaller studies often cannot: differences in overall survival across diverse racial and ethnic groups.
Why disaggregating data matters
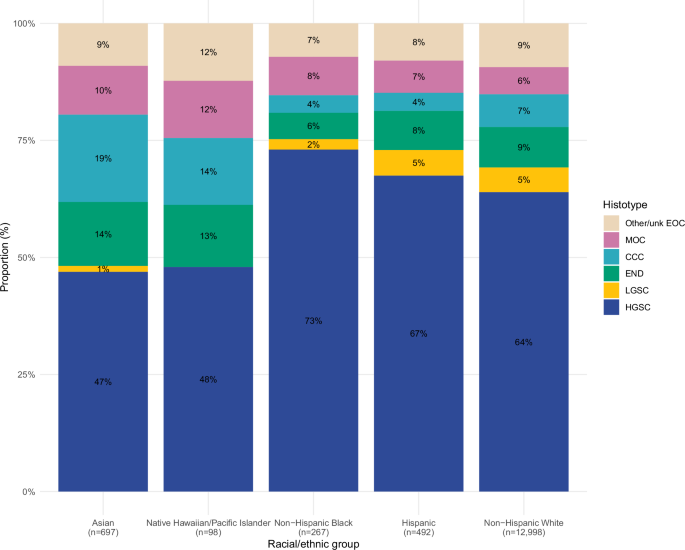
Historically, studies of ovarian cancer survival have grouped populations in ways that obscure important differences. One key example is the combining of Asian and Native Hawaiian and Pacific Islander women into a single category. This approach risks masking disparities.
In our study, we made a deliberate effort to separate Asian and Native Hawaiian and Pacific Islander groups. This required requesting original data sources, incorporating self-reported racial and ethnic groups and genetic ancestry when necessary. The result was a clearer, more nuanced picture—one that revealed important differences that had previously been hidden.
Unequal outcomes across populations
The key finding was clear: survival after ovarian cancer diagnosis is not equal across racial and ethnic groups.
Compared with non-Hispanic White women, we found significantly poorer survival among non-Hispanic Black women and, most notably, Native Hawaiian and Pacific Islander women. Native Hawaiian and Pacific Islander women had around a 1.6-fold higher risk of death, while non-Hispanic Black women had about a 1.3-fold higher risk. These disparities persisted even after accounting for established prognostic factors such as age, tumour type, and stage at diagnosis.
In contrast, Asian women tended to have similar or slightly better survival compared with non-Hispanic White women. This contrast is particularly important: if Asian and Native Hawaiian and Pacific Islander women are analysed together, the poorer outcomes for Pacific Islander women may be overlooked entirely.
What might be driving these differences?
Understanding why these disparities exist is complex. Our analysis accounted for a range of clinical and lifestyle factors, including body mass index, smoking, and hormone use, but these did not fully explain the observed differences.
This points to broader structural and systemic factors. Previous research suggests that differences in access to care, availability of specialist treatment, and adherence to clinical guidelines can all influence survival outcomes. Social determinants of health—such as socioeconomic status, geography, and historical inequities—are also likely to play an important role.
For Native Hawaiian and Pacific Islander populations in particular, geographical isolation and healthcare workforce shortages may contribute to reduced access to timely and high-quality care. Our study could not directly measure these factors, but the patterns we observed strongly suggest their influence and highlight important future areas of investigation.
The challenge—and power—of global collaboration
A major strength of this work lies in its scale. Pooling data from 18 studies allowed us to include populations that are often underrepresented in cancer research, such as Native Hawaiian and Pacific Islander women.
However, this approach also comes with challenges. Not all studies collected the same variables, and information on treatment, comorbidities, and socioeconomic factors was limited. These are precisely the factors we need to better understand the pathways leading to disparities.
Despite these limitations, the ability to harmonise and analyse such a large and diverse dataset demonstrates the power of international collaboration. For rare cancers like ovarian cancer—and particularly for less common populations—this kind of approach is essential.
Moving forward: from evidence to action
Our findings highlight a clear message: improving ovarian cancer outcomes requires more than advances in biology and treatment. It also demands attention to equity.
First, future research must continue to disaggregate data. Grouping populations too broadly can conceal important differences and delay action where it is most needed.
Second, we need better data on healthcare access, treatment pathways, and social determinants of health. Without this, it is difficult to identify specific interventions that may have the greatest impact.
Finally, there is a need for targeted efforts across research to address disparities. This includes a need to broaden these powerful international consortia resources further to represent more diverse populations. This will hopefully lead to an improved understanding of the deeper issues driving inequity and assist to find solutions to improve outcomes for all.
Follow the Topic
-
British Journal of Cancer
This journal is devoted to publishing cutting edge discovery, translational and clinical cancer research across the broad spectrum of oncology.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in