Reprogramming the breast tumor immune microenvironment: cold-to-hot transition for enhanced immunotherapy
Published in Cancer, Cell & Molecular Biology, and General & Internal Medicine
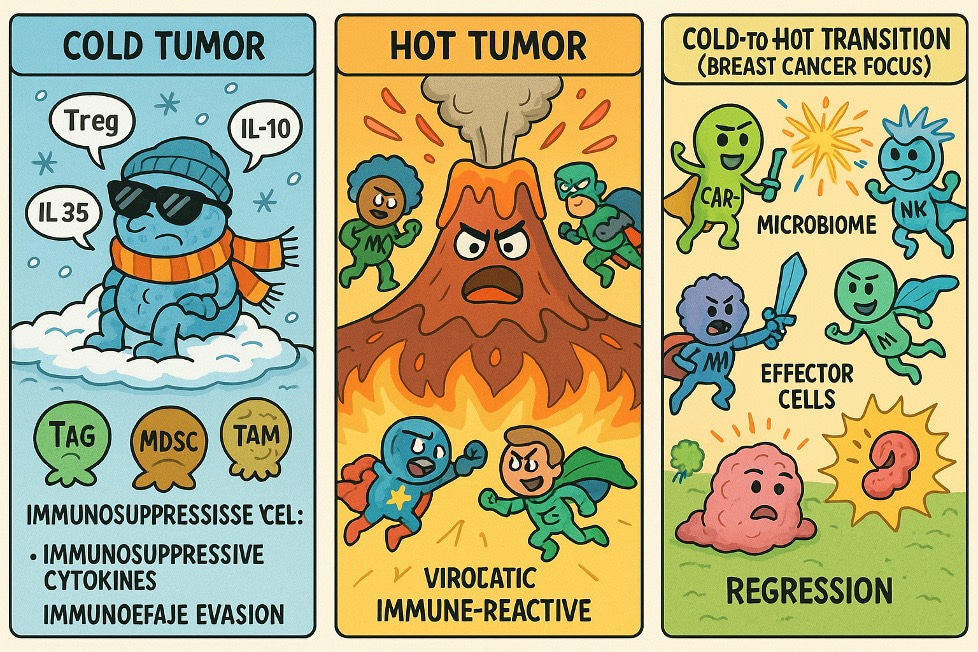

This review explores how the immunosuppressive TME in breast cancer blocks effective immune activation and impairs immunotherapy 1. Dominant immune-suppressive cells- Tregs, MDSCs, and TAMs—release cytokines such as IL-35, IL-10, and TGF-β, which contribute to T cell exclusion and dysfunction 2. We discuss how this immune barrier is particularly pronounced in hormone receptor-positive and triple-negative subtypes 1. Emerging interventions—including checkpoint blockade, mRNA vaccines, and oncolytic viruses—aim to remodel the TME and support cold-to-hot tumor transformation for improved immunotherapeutic response 3.
The Need for Reprogramming the TME
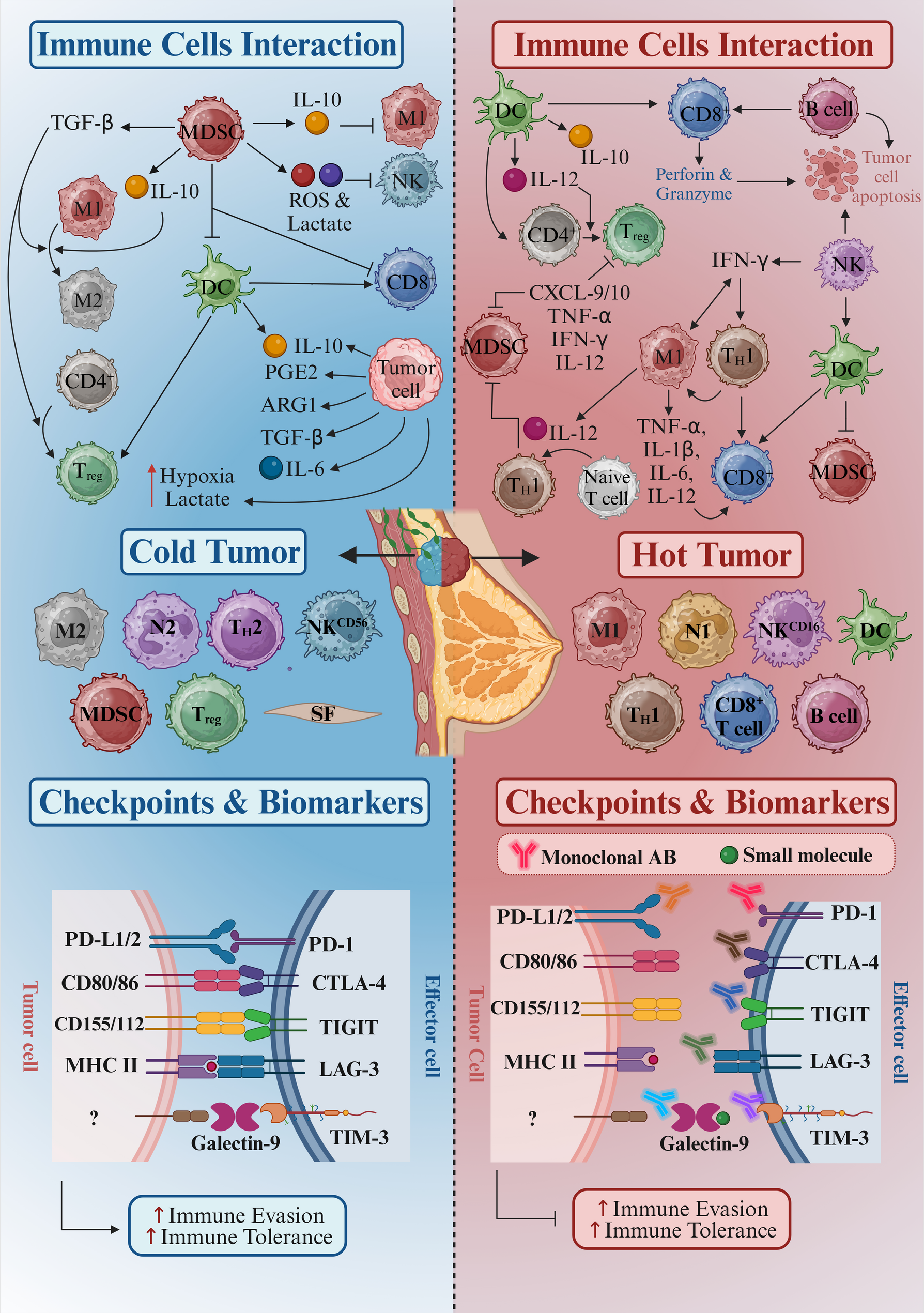
The breast cancer TME typically lacks sufficient immune infiltration and is dominated by suppressive cells that block antitumor immunity. Tregs, MDSCs, and TAMs disrupt immune activation, while poor antigen presentation and high levels of checkpoint receptors like PD-1, TIGIT, and LAG-3 further restrict T cell function 4,5. Reprogramming this environment is essential to drive a shift toward a “hot” TME. Doing so enhances cytotoxic T cell access and activity, enabling immunotherapies to overcome resistance and achieve better clinical outcomes 6-8.
Advancements and Scientific Significance
Recent advancements in breast cancer immunotherapy have focused on overcoming the cold TME 9. ICIs targeting PD-1, LAG-3, and TIGIT have shown promise, particularly when combined with therapies that induce immunogenic cell death or enhance immune cell activation, such as CAR T-cell therapies. mRNA vaccines have emerged as a potential tool to enhance T cell responses by increasing antigen presentation 10. These strategies, when used together, aim to convert the immunologically inert TME into a more active one, improving the overall efficacy of immunotherapies 11.
Inspiration for the Study
This review is inspired by recent advances in cancer immunotherapy and the evolving understanding of the TME, particularly the role of the microbiome 1. Emerging evidence indicates that both gut and tumor-associated microbiota significantly shape systemic and local immune responses, influencing the efficacy of immunotherapies across various cancer types, including breast cancer 12-14. Another key development is the identification of neo-antigens—tumor-specific peptides generated from somatic mutations—which provide promising targets for personalized immunotherapy. mRNA-based vaccines targeting clonal neo-epitopes, such as those derived from PIK3CA, TP53, or ESR1 mutations, have demonstrated the capacity to enhance cytotoxic CD8+ T cell responses and improve tumor recognition 15-18.
Importantly, these approaches are particularly relevant given the molecular heterogeneity of breast cancer. In HR+/HER2– tumors, often driven by ESR1 mutations and enriched in luminal gene expression profiles, the TME is characterized by low MHC-I expression and minimal CD8+ T cell infiltration. Heating strategies in this context may include STING agonists or IL-2 variants to promote dendritic cell activation and T cell recruitment. In HER2+ subtypes, frequently associated with ERBB2 amplification, resistance to trastuzumab has been linked to immune escape mechanisms such as PD-L1 upregulation; thus, mRNA vaccines encoding HER2-derived neoepitopes or co-administration with GM-CSF may potentiate immune activation. Triple-negative breast cancer (TNBC), often harboring TP53 mutations and basal-like signatures, displays elevated tumor-infiltrating lymphocytes (TILs) and PD-L1 expression, making it amenable to immune checkpoint blockade. Nonetheless, immune efficacy may be further enhanced through mRNA vaccines targeting clonal neoantigens or shared tumor-associated antigens (TAAs) such as NY-ESO-1 or MAGE-A, especially when coupled with microbiome modulation using Bifidobacterium or Faecalibacterium 19,20.
The concept of “heating” the TME—converting immune-cold or excluded tumors into inflamed, T cell–rich environments—enables a paradigm shift from passive to active immunotherapy. By integrating neoantigen prediction, microbiota engineering, and mRNA vaccine platforms, even immunologically inert subtypes may be sensitized to advanced immunotherapeutic modalities, including mesothelin-targeted CAR-T cells, cancer stem-like cell-directed therapies, CTLA-4 blockade, and next-generation neoantigen-based mRNA vaccines across the molecular spectrum of breast cancer 21-23.
Future Directions
Reprogramming the TME from cold to hot involves boosting immune cell infiltration and overcoming the immunosuppressive barriers that limit the effectiveness of therapies like ICIs. In cold tumors, such as TNBC, the TME is typically hostile to immune cells, with immune-excluded regions dominated by Tregs, MDSCs, and TAMs. These suppressive cells hinder immune activation and allow the tumor to evade immune surveillance 7.
Targeting these immune-suppressive cells directly is essential. For example, therapies aimed at depleting Tregs or blocking MDSC activity can make the TME more permissive to immune cell infiltration. Additionally, addressing stromal factors like hypoxia and lactate accumulation, which promote immune suppression, can further help "Heat-Up" the TME by improving the conditions for immune cells to thrive 11.
In TNBC, which often lacks effective immune responses, reprogramming the TME is crucial. This can be achieved by targeting the suppressive elements within the TME, making the tumor more vulnerable to immune activation. Strategies like combining TME modulation with mRNA vaccines or oncolytic virus therapy could further enhance immune responses, especially in TNBC, which otherwise resists conventional treatments 24,25.
Immunosculpting, the process by which tumors establish niches that shape immune responses, plays a significant role in cold tumor resistance. TNBC and other subtypes exploit these niches to prevent immune cells from infiltrating or recognizing the tumor. Novel approaches are being explored to target these immune-excluded regions with immunostimulatory agents, thereby increasing immune activation within the tumor .
In luminal breast cancer, chemotherapy-induced cell death (ICD) has shown promise in transforming cold tumors to hot ones by inducing immune responses. However, resistance remains a challenge, particularly in HER2-positive cancers, where tumors can shed HER2 or activate immune checkpoints like PD-L1, which blocks the immune response. To combat this, combination therapies—such as pairing ICIs with chemotherapy or targeted therapies—are being tested to overcome these mechanisms of resistance 26-28.
The future of breast cancer treatment lies in refining strategies to modulate the TME effectively. Key directions include developing therapies targeting alternative immune checkpoints, such as LAG-3 and TIGIT, which could enhance immune responses. Additionally, improving patient selection through better biomarkers will ensure that therapies are directed to those who will benefit the most 29,30. By addressing the complexity of the TME and immune resistance mechanisms, these approaches can potentially transform the landscape of breast cancer immunotherapy.
Summary
This paper emphasizes the importance of reprogramming the TME to overcome immune exclusion and resistance in breast cancer. Combining immune checkpoint inhibitors, CAR T-cell therapies, and mRNA vaccines, strategies are emerging that can convert cold tumors into hot, immunologically responsive ones. These therapies offer hope for improving patient outcomes, especially for difficult-to-treat subtypes like HR+, TNBC, and HER2+ breast cancer.
About Authors
Saber Imani is an independent Assistant Professor at Shulan International Medical College, Zhejiang Shuren University, Hangzhou, China. He leads a research lab advancing mRNA-based cancer vaccines and translational oncology. His work focuses on unraveling the molecular mechanisms underlying cancer and viral diseases, with particular emphasis on ICIs and the role of immunotherapy in cancer treatment. Through his leadership, his lab critically contributes to developing innovative cancer therapies, aiming to reprogram the TME for enhanced anti-tumor responses. By targeting key immunological pathways and advancing strategies like ICI-based therapy and mRNA vaccination, his research holds the potential to address global health challenges and improve cancer treatment outcomes.
Ghazaal Roozitalab is a surgical assistant who graduated with a degree in anesthesia nursing from Fasa University of Medical Sciences. Passionate about integrating clinical practice with cutting-edge research, her interests span nano‑drug delivery systems, cancer immunotherapy, and biotechnology. Driven by curiosity, Ghazaal adopts a question-oriented approach to pinpoint gaps in scientific knowledge and inspire innovative solutions. In close collaboration with Dr. Parham Jabbarzadeh Kaboli, she contributes to multiple interdisciplinary projects to advance targeted cancer therapies.
Mazaher Maghsoudloo holds a PhD in Bioinformatics from Tehran University, where he graduated in 2020. With a background in Computer Science, he combines computational expertise with a deep understanding of biological systems. Since 2023, he has been serving as a Research Associate at Southwest Medical University, working in the Key Laboratory of Epigenetics and Oncology within the Research Center for Preclinical Medicine. His research focuses on cancer biology, particularly on biomarker detection and the reconstruction of disease networks, with a special emphasis on cancer-related applications. He works closely with Dr. Saber Imani, and together they lead collaborative efforts in advancing mRNA-based cancer vaccines, translational oncology, and research on various cancers, emphasizing ICIs and immunotherapy. Through this collaboration, they aim to reprogram the TME and develop innovative therapeutic strategies to enhance anti-tumor responses and improve cancer treatment outcomes.
Parham Jabbarzadeh Kaboli is a dedicated cancer researcher based in the United States. He earned his Ph.D. in Pharmacology from Universiti Putra Malaysia in 2018 and maintains an h-index of 25 with over 1,900 citations. His research primarily centers on developing targeted therapies and uncovering resistance mechanisms in breast cancer. Dr. Kaboli has published impactful studies, mentored emerging scientists, and worked under distinguished mentors in Malaysia, China, Taiwan, and the U.S. During his postdoctoral fellowship at China Medical University in Taiwan, he conducted pioneering research on the c-MET receptor tyrosine kinase. Aiming to overcome drug resistance in solid tumors, Dr. Kaboli plans to establish a research program that integrates immunotherapy with clinical applications. He remains committed to training the next generation of scientists and excels in cross-cultural collaboration.
References
- Imani, S., et al. Reprogramming the breast tumor immune microenvironment: cold-to-hot transition for enhanced immunotherapy. Journal of Experimental & Clinical Cancer Research 44, 131 (2025).
- Petrosyan, V., et al. Immunologically "cold" triple negative breast cancers engraft at a higher rate in patient derived xenografts. NPJ Breast Cancer 8, 104 (2022).
- Lin, X., et al. Combination of CTLA-4 blockade with MUC1 mRNA nanovaccine induces enhanced anti-tumor CTL activity by modulating tumor microenvironment of triple negative breast cancer. Transl Oncol15, 101298 (2022).
- Shi, W., et al. Next-generation anti-PD-L1/IL-15 immunocytokine elicits superior antitumor immunity in cold tumors with minimal toxicity. Cell Rep Med 5, 101531 (2024).
- Choi, W., Lee, J., Lee, J., Lee, S.H. & Kim, S. Hepatocyte Growth Factor Regulates Macrophage Transition to the M2 Phenotype and Promotes Murine Skeletal Muscle Regeneration. Front Physiol 10, 914 (2019).
- Yang, Y., et al. An Oncolytic Adenovirus Targeting Transforming Growth Factor beta Inhibits Protumorigenic Signals and Produces Immune Activation: A Novel Approach to Enhance Anti-PD-1 and Anti-CTLA-4 Therapy. Hum Gene Ther 30, 1117-1132 (2019).
- Zhou, Z., et al. Infiltrating treg reprogramming in the tumor immune microenvironment and its optimization for immunotherapy. Biomark Res 12, 97 (2024).
- Sasidharan Nair, V., et al. DNA methylation and repressive H3K9 and H3K27 trimethylation in the promoter regions of PD-1, CTLA-4, TIM-3, LAG-3, TIGIT, and PD-L1 genes in human primary breast cancer. Clin Epigenetics 10, 78 (2018).
- Papakonstantinou, A., et al. The conundrum of breast cancer and microbiome - A comprehensive review of the current evidence. Cancer Treat Rev 111, 102470 (2022).
- Liu, Z., et al. Engineering neoantigen vaccines to improve cancer personalized immunotherapy. Int J Biol Sci 18, 5607-5623 (2022).
- Liu, Z., et al. Immunosuppression in tumor immune microenvironment and its optimization from CAR-T cell therapy. Theranostics 12, 6273-6290 (2022).
- Kaboli, P.J., Roozitalab, G., Farghadani, R., Eskandarian, Z. & Zerrouqi, A. c-MET and the Immunological Landscape of Cancer: Novel Therapeutic Strategies for Enhanced Anti-Tumor Immunity. Front. Immunol. 15(2024).
- Laborda-Illanes, A., et al. Breast and Gut Microbiota Action Mechanisms in Breast Cancer Pathogenesis and Treatment. Cancers (Basel) 12(2020).
- Chen, J., et al. The microbiome and breast cancer: a review. Breast Cancer Res Treat 178, 493-496 (2019).
- Roozitalab, G., Abedi, B., Imani, S., Farghadani, R. & Jabbarzadeh Kaboli, P. Comprehensive assessment of TECENTRIQ® and OPDIVO®: analyzing immunotherapy indications withdrawn in triple-negative breast cancer and hepatocellular carcinoma. Cancer Metastasis Rev 43, 889-918 (2024).
- Peng, W., et al. Loss of PTEN Promotes Resistance to T Cell-Mediated Immunotherapy. Cancer Discov6, 202-216 (2016).
- Sharma, P., Hu-Lieskovan, S., Wargo, J.A. & Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 168, 707-723 (2017).
- Hanna, A. & Balko, J.M. Breast cancer resistance mechanisms: challenges to immunotherapy. Breast Cancer Res Treat 190, 5-17 (2021).
- Maher, V.E., et al. Analysis of the Association Between Adverse Events and Outcome in Patients Receiving a Programmed Death Protein 1 or Programmed Death Ligand 1 Antibody. J Clin Oncol 37, 2730-2737 (2019).
- Al-Ansari, M.M., AlMalki, R.H., Dahabiyeh, L.A. & Abdel Rahman, A.M. Metabolomics-Microbiome Crosstalk in the Breast Cancer Microenvironment. Metabolites 11(2021).
- Parra, K., et al. Impact of CTLA-4 blockade in conjunction with metronomic chemotherapy on preclinical breast cancer growth. Br J Cancer 116, 324-334 (2017).
- Lei, X., et al. A Pan-Histone Deacetylase Inhibitor Enhances the Antitumor Activity of B7-H3-Specific CAR T Cells in Solid Tumors. Clin Cancer Res 27, 3757-3771 (2021).
- Wang, Z., et al. Phase I study of CAR-T cells with PD-1 and TCR disruption in mesothelin-positive solid tumors. Cell Mol Immunol 18, 2188-2198 (2021).
- Chuangchot, N., et al. Enhancement of PD-L1-attenuated CAR-T cell function through breast cancer-associated fibroblasts-derived IL-6 signaling via STAT3/AKT pathways. Breast Cancer Res 25, 86 (2023).
- Tchou, J., et al. Safety and Efficacy of Intratumoral Injections of Chimeric Antigen Receptor (CAR) T Cells in Metastatic Breast Cancer. Cancer Immunol Res 5, 1152-1161 (2017).
- Zhou, Z., et al. Emerging role of immunogenic cell death in cancer immunotherapy: Advancing next-generation CAR-T cell immunotherapy by combination. Cancer Lett 598, 217079 (2024).
- Yang, L., Hu, Q. & Huang, T. Breast Cancer Treatment Strategies Targeting the Tumor Microenvironment: How to Convert "Cold" Tumors to "Hot" Tumors. Int J Mol Sci 25(2024).
- Tabana, Y., Okoye, I.S., Siraki, A., Elahi, S. & Barakat, K.H. Tackling Immune Targets for Breast Cancer: Beyond PD-1/PD-L1 Axis. Front Oncol 11, 628138 (2021).
- Fang, J., et al. Prognostic value of immune checkpoint molecules in breast cancer. Biosci Rep40(2020).
- Koyama, S., et al. Adaptive resistance to therapeutic PD-1 blockade is associated with upregulation of alternative immune checkpoints. Nat Commun 7, 10501 (2016).
Follow the Topic
-
Journal of Experimental & Clinical Cancer Research
Journal of Experimental & Clinical Cancer Research is an online peer-reviewed journal that publishes original research papers, reviews and commentaries in cancer research, from bench to bedside.

Related Collections
With Collections, you can get published faster and increase your visibility.
Insights into the relationship between metabolism and cancer
Cancer metabolism has become one of the most studied aspects of the "hallmarks of cancer." It refers to alterations in how tumor cells process nutrients to fuel their rapid proliferation and spread. These dramatic dysregulations include elevated glucose uptake even in the presence of oxygen (the Warburg effect), dependence on glutamine, and the production of waste products such as lactate, which further support tumor growth and metastasis. Genetic mutations accumulating during cancer progression in metabolic enzymes and cancer-promoting signaling pathways directly affect metabolic changes in cancer cells as well as in the tumor microenvironment [1,2].
A growing number of scientists are developing targeted therapies to exploit these metabolic differences to slow or halt cancer progression. Some therapies aim to block or alter the production of specific metabolites, while several drugs for other pathologies, such as diabetes, are of great interest due to their potential to slow tumor growth by altering systemic metabolic factors such as insulin and glucose levels in a "drug repositioning" strategy [3-7].
Cancer metabolism, involving altered lipid, iron, and amino acid pathways, regulates ferroptosis, an iron-dependent, lipid peroxidation-driven form of cell death. Cancer cells often resist this process, but targeting their specific metabolic vulnerabilities, such as glutathione depletion or iron overload, can trigger ferroptosis to kill tumor cells and overcome drug resistance [8].
Cancer cells can rewire their metabolism when one pathway is blocked, so it is becoming clear that combining metabolism inhibitors with traditional chemotherapy, radiotherapy, or immunotherapy may be an effective therapeutic strategy [8]. While some metabolism-targeting drugs have been successful (e.g., in Acute Lymphocytic Leukemia), targeting cancer metabolism is complex due to its similarity to normal cell processes [9]. Metabolic profiling of patients is helping to identify specific vulnerabilities, leading to more personalized metabolic therapies [10].
Understanding cancer metabolism at a deeper mechanistic level is also essential to improving immunotherapy, as immune cell metabolism changes during therapy administration, contributing to acquired resistance.
KEYWORDS: metabolomics; proteomics, genomics, mitochondrial metabolism, ferroptosis, oxidative stress, inflammation, innovative study models, new translational therapeutic approaches.
In this Collection of the Journal of Experimental & Clinical Cancer Research, we would like to promote studies that further dissect the molecular mechanisms through which cancer cells reprogram their own metabolism and that of cells in the tumor microenvironment, thus driving disease progression. Furthermore, studies that highlight potential metabolic vulnerabilities that could be targeted therapeutically will be of interest.
References
- Finley LWS. What is cancer metabolism? Cell. 2023;186(8):1670-88. PubMed PMID: 36858045. PMCID: PMC10106389.eng
- Guertin DA, Wellen KE. Acetyl-CoA metabolism in cancer. Nat Rev Cancer. 2023;23(3):156. PubMed PMID: 36658431. PMCID: PMC11137663.eng
- Vander Heiden MG. Targeting cancer metabolism: a therapeutic window opens. Nat Rev Drug Discov. 2011;10(9):671-84. PubMed PMID: 21878982.
- Zou W, Han Z, Wang Z, Liu Q. Targeting glutamine metabolism as a potential target for cancer treatment. J Exp Clin Cancer Res. 2025;44(1):180. PubMed PMID: 40598593. PMCID: PMC12210561.
- Formenti L, Abramo F, Dellavedova G, Dematteis V, Decio A, Grasselli C, et al. Impairment of oxidative metabolism compromises Rad51 recruitment and potentiates PARP inhibitor effectiveness in ovarian cancer. J Exp Clin Cancer Res. 2026;45(1):45. PubMed PMID: 41530766. PMCID: PMC12888472.
- Chen T, Xu ZG, Luo J, Manne RK, Wang Z, Hsu CC, et al. NSUN2 is a glucose sensor suppressing cGAS/STING to maintain tumorigenesis and immunotherapy resistance. Cell Metab. 2023;35(10):1782-98.e8. PubMed PMID: 37586363. PMCID: PMC10726430.
- Pillai U J, Ray A, Maan M, Dutta M. Repurposing drugs targeting metabolic diseases for cancer therapeutics. Drug Discov Today. 2023;28(9):103684. PubMed PMID: 37379903.
- Wu Y, Li H, Yue K, Jing C, Duan Y. Ferroptosis in cancer: metabolism, mechanisms and therapeutic prospects. Mol Cancer. 2025;24(1):303.
- Punnasseril JMJ, Auwal A, Gopalan V, Lam AK, Islam F. Metabolic Reprogramming of Cancer Cells and Therapeutics Targeting Cancer Metabolism. Cancer Med. 2025;14(18):e71244. PubMed PMID: 40956032. PMCID: PMC12439291.
- da Silva-Diz V, Herranz D. Unleashing the Full Potential of Metabolic Interventions in T-ALL. Blood Cancer Discov. 2025;6(3):163-7. PubMed PMID: 40111138. PMCID: PMC12050939.
- Benjamin DI, Cravatt BF, Nomura DK. Global profiling strategies for mapping dysregulated metabolic pathways in cancer. Cell Metab. 2012;16(5):565-77. PubMed PMID: 23063552. PMCID: PMC3539740.
Publishing Model: Open Access
Deadline: Feb 28, 2027


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in