SARS-Cov-2 infection in newborns: cord blood IgA/IgM suggest in utero infection is more common than previously thought
Published in Microbiology, General & Internal Medicine, and Paediatrics, Reproductive Medicine & Geriatrics
In the first year of the COVID-19 pandemic, the news was dominated by the impact of COVID-19 on the elderly. Children, especially newborns, were not considered to be at risk and pediatric COVID-19 cases were largely ignored. Naso-pharyngeal swab tests were developed primarily for adult patients, and their painful nature was not suitable for the routine surveillance of the younger population. In response, we began the development of our own assay, one that could be used for both adults and children: a saliva test. With this, we started to research pediatric COVID-19 and enrolled mothers and their infants into a long-term study.
In August 2020, a newborn participant that had been enrolled in our study by the mother was transferred immediately after birth to the Neonatal Intensive Care Unit (NICU) at Los Angeles General Medical Center. The infant showed COVID-19 symptoms on the day of birth. We found a high viral load in the newborn saliva. Considering the incubation time of SARS-CoV-2, we suspected the newborn infection predated delivery. Meanwhile, similar cases were reported worldwide. Shortly after, another patient from our study was transferred to the NICU with high viral load at birth. We asked ourselves: could in utero transmission be more frequent than previously thought?
A major obstacle was the lack of available testing. Even RT-PCR, the gold standard, could easily miss babies with in utero infection. Indeed, after an incubation time, viral load typically peaks then decreases over a few weeks. This means we would only detect in utero transmission if the infection occurs within a week or two before delivery. For many congenital infections, in utero transmission is assessed using serology. Unfortunately, at the time, serological tests were rare and focused on only one type of antibody (isotype): the long-lasting IgG from adult samples.
IgG are small antibodies that the mother transfers to the newborn via the placenta. The fetus can also produce their own IgG if an infection occurs late in the pregnancy. IgM and IgA antibodies are different. IgM is transient and is the first antibody produced in response to an infection. IgA takes longer to arise, but is more specific, and lasts longer. IgA antibodies offer better protection, especially in the mucosa. Importantly, both IgM and IgA are multimeric, bulkier antibodies that do not cross the placenta. Their presence at birth generally indicates that the fetus had an immune response to in utero infection or exposure in the last trimester.
With this in mind, we decided to develop our own assay to test for fetal IgM and IgA. We modified a SARS-CoV-2 IgG assay, that the FDA had recently approved under an emergency use authorization (EUA), so it could also specifically detect IgM and IgA. We then validated our modified assay for cord blood samples using commercial control samples and an international standard obtained from the World Health Organization. We also used our laboratory cord blood repository from patients enrolled in other studies before SARS-CoV-2 emergence as true negative samples to help validate the assay and determine the cut off for positivity.
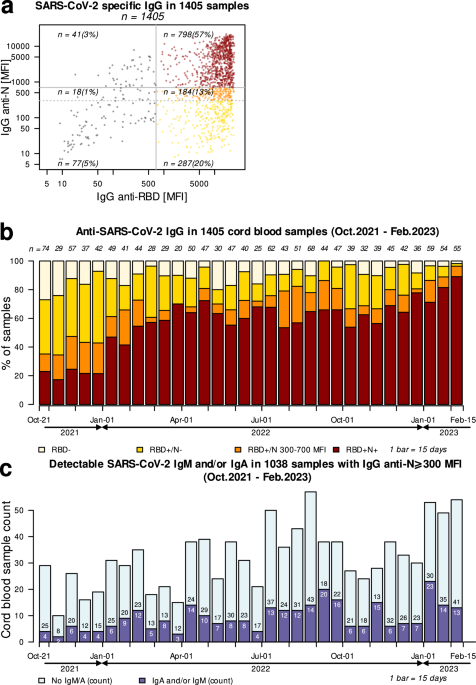
We obtained remnant cord blood samples from the blood bank at the Los Angeles General Medical Center between October 2021 and February 2023.We studied 1405 infants which represented over 90% of all infants born at Los Angeles General Medical Center during that time. These cord blood samples were tested for IgG, IgM, and IgA. The IgG, shared between the mothers and the newborns, were important to give us an overview of the COVID-19 pandemic in the Los Angeles area: we measured antibodies targeting the viral protein Nucleocapsid (found only in participants that had been infected) and the Receptor Binding Domain (RBD) of the Spike glycoprotein, found after both viral infection and vaccination. Not surprisingly, we saw overtime more and more participants were positive for anti-RBD (as a mass vaccination campaign was underway), and positive for both anti-RBD and anti-N (indicating that more and more people had been infected).
We then tested IgM and IgA in cord blood samples that had IgG anti-N above background level. This time, the results were unexpected: more than a quarter of the newborns had IgM and/or IgA in their cord blood, indicating immune response to in utero exposure. During the study period we also found that as new variants emerged and became the dominant strain, we saw variation in the numbers of infants with detectable IgA or IgM antibodies indicating that some variants may be more likely to infect the newborn.
Serology is often used to identify vertical transmission of other pathogens (Toxoplasmosis, CMV, Zika Virus), but requires confirmational testing which would call for follow-up testing of infants thought to have potential in utero infection, which was not available for this study. But these early results raise an important question concerning the long-term effects of potential in utero infection among newborns with presence of IgA and/or IgM antibodies to SARS-CoV-2. The infections cited above have been shown to impact the newborn’s health, with outcomes including microcephaly and malformations. In the case of COVID-19, what will be the long-term consequences? SARS-CoV-2 is known to impact not only the respiratory tract, but also the cardiovascular system, the immune system, as well as the brain. And there remain a lot of unknowns regarding long-COVID. In this study we found that 25% of newborns tested had evidence of in utero immune response to SARS-CoV-2. Thus, it is critical that there is further investigation of the short- and long-term outcomes of these infants.
I am a virologist with over 15 years of research experience in the field of emerging zoonotic viruses, with a special attention on bat-borne diseases (Nipah Virus, Ebola Virus, SARS-CoV 1 and 2, ...). I am especially interested in host-virus interactions and how to use them for biomedical applications (drug discovery, gene therapy, high-throughput serology, outbreak preparedness...).
I am currently an Assistant Professor at Keck Medicine of USC (Pediatrics) conducting clinical and translational research focusing on SARS-CoV-2 in newborns. I am also teaching Virology (MIMG 102 XL) and Cell& Molecular Biology (LS 7A XL) at UCLA and serve as President for EnViro International Laboratories.
Follow the Topic
-
Nature Communications
An open access, multidisciplinary journal dedicated to publishing high-quality research in all areas of the biological, health, physical, chemical and Earth sciences.

Related Collections
With Collections, you can get published faster and increase your visibility.
Women's Health
Publishing Model: Hybrid
Deadline: Ongoing
Biosensing
Publishing Model: Hybrid
Deadline: Jun 30, 2026



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in
Excellent study. This is a great foundation for further work, especially regarding the growing number of patients with LONG COVID.