Severe resistant hypercalcemia complicating rhabdomyolysis: recognizing a rare and prolonged metabolic complication
Published in Biomedical Research
Explore the Research
Severe resistant hypercalcemia complicating rhabdomyolysis: a case report and review of the literature
Why this case matters
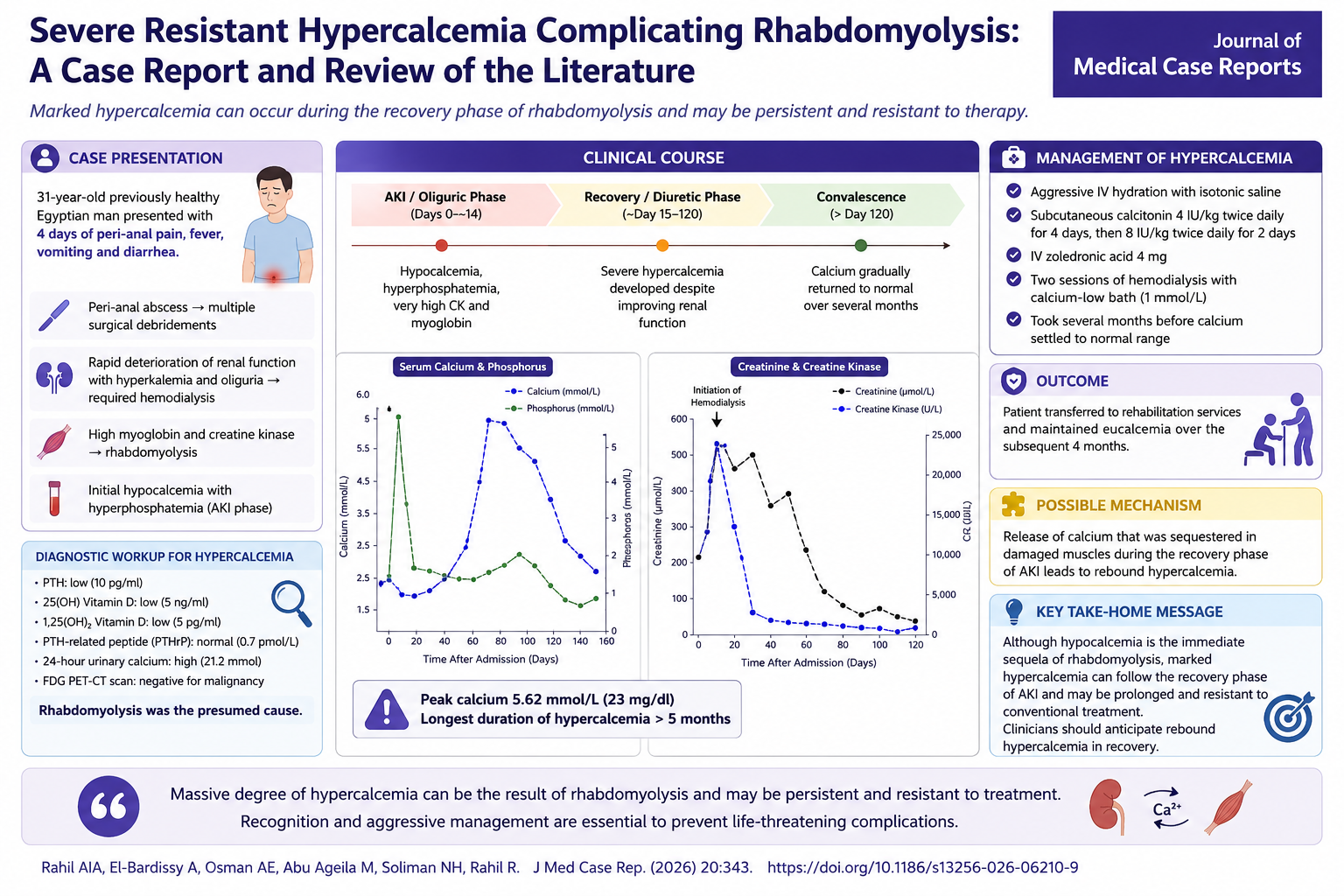
Rhabdomyolysis is classically associated with hypocalcemia during the acute phase, making subsequent severe hypercalcemia an easily overlooked complication. This case describes a previously healthy 31-year-old man who developed profound, treatment-resistant hypercalcemia (peak corrected calcium 5.62 mmol/L [23 mg/dL]) several weeks after recovering from rhabdomyolysis-induced acute kidney injury. Extensive investigation excluded common causes of PTH-independent hypercalcemia, supporting delayed calcium release from injured skeletal muscle as the underlying mechanism.
The patient required aggressive management including intravenous hydration, repeated calcitonin therapy, zoledronic acid, and low-calcium hemodialysis, yet normalization of calcium required approximately five months. The authors note that this represents one of the highest reported calcium levels and among the most prolonged recoveries described following rhabdomyolysis.
Key clinical insights
- Hypercalcemia may occur weeks after apparent recovery from rhabdomyolysis and acute kidney injury.
- Recovery follows a characteristic biphasic calcium pattern, with early hypocalcemia followed by delayed rebound hypercalcemia.
- Severe hypercalcemia may persist despite conventional therapy and require dialysis in addition to antiresorptive treatment.
- Suppressed parathyroid hormone, low vitamin D metabolites, normal PTH-related peptide, and exclusion of malignancy help establish the diagnosis.
- Serial monitoring of calcium during recovery may prevent unnecessary diagnostic investigations and facilitate earlier intervention.
Clinical Take-Home Message
Although hypocalcemia is expected during the acute phase of rhabdomyolysis, clinicians should remain vigilant for delayed, potentially profound rebound hypercalcemia during recovery. Continued biochemical surveillance after improvement in renal function is essential, as severe cases may require prolonged, multimodal therapy before spontaneous resolution occurs.
Multiple Choice Question
A patient recovering from rhabdomyolysis-associated acute kidney injury develops severe hypercalcemia 4 weeks after normalization of renal function. Laboratory evaluation reveals suppressed parathyroid hormone (PTH), low 25-hydroxyvitamin D, low 1,25-dihydroxyvitamin D, normal PTH-related peptide (PTHrP), and no evidence of malignancy. What is the most likely mechanism of the hypercalcemia?
A. Primary hyperparathyroidism with autonomous PTH secretion
B. Malignancy-related secretion of PTHrP
C. Release of calcium previously sequestered in damaged skeletal muscle during recovery from rhabdomyolysis
D. Vitamin D intoxication
Correct Answer
C. Release of calcium previously sequestered in damaged skeletal muscle during recovery from rhabdomyolysis
Explanation
During the acute phase of rhabdomyolysis, calcium is deposited within injured skeletal muscle, resulting in hypocalcemia. As muscle heals and renal function recovers, this sequestered calcium is gradually released back into the circulation, producing delayed hypercalcemia. In severe cases, the hypercalcemia may be profound, prolonged, and resistant to standard therapies, as demonstrated in this case report. Recognition of this characteristic biphasic disturbance in calcium homeostasis can prevent unnecessary evaluation for malignancy or endocrine disorders and emphasizes the importance of continued calcium monitoring during recovery.
- A is incorrect: Primary hyperparathyroidism is characterized by an inappropriately normal or elevated PTH level, not a suppressed PTH.
- B is incorrect: Humoral hypercalcemia of malignancy is associated with elevated PTHrP and typically evidence of an underlying malignancy.
- D is incorrect: Vitamin D intoxication produces elevated 25-hydroxyvitamin D (and often elevated 1,25-dihydroxyvitamin D), findings not present in this patient.
Journal of Medical Case Reports is the world's first international, PubMed-listed medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports. The journal is open access and strongly endorses the CARE guidelines for case reports, requiring authors to submit populated CARE checklists with submissions to improve transparency in reporting.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.



![When PSMA-targeted therapy is not enough: high-risk localized prostate cancer after repeated [177Lu]Lu-PSMA radioligand therapy](/cdn-cgi/image/metadata=copyright,fit=scale-down,format=auto,quality=95,width=256,height=256/https://public-storage.zapnito.com/Ku6h7Yyp4Q0LXqRRMICCHR2v4LcOsmxMrmDPtOYuI1c)

Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in