Targeting DCPS in myeloid malignancies: The path from biomarker discovery to clinical utility
Published in Cancer, Biomedical Research, and Pharmacy & Pharmacology


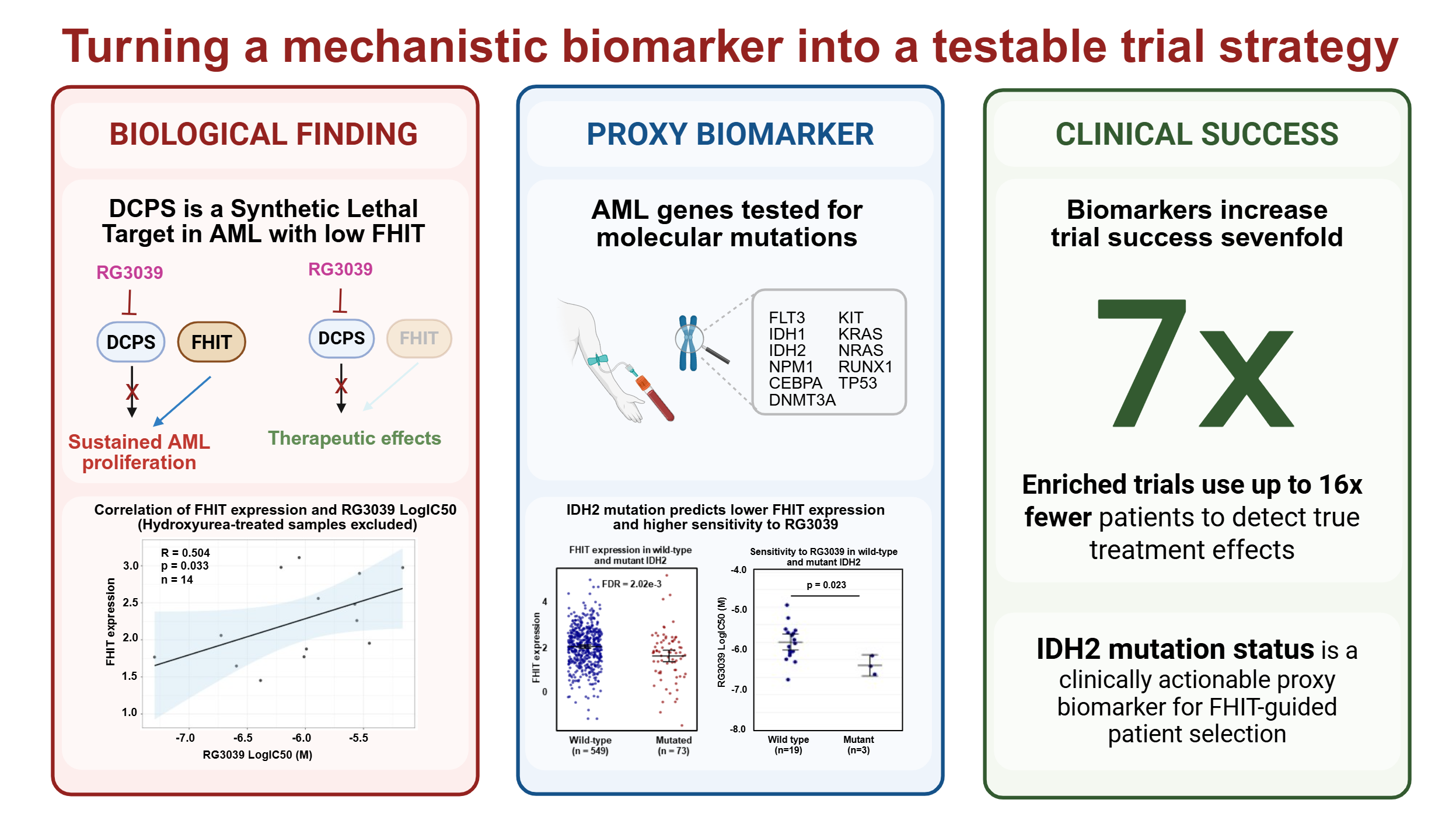
We previously published a link between Acute Myeloid Leukemia cells expressing low levels of the tumor suppressor FHIT and sensitivity to loss of the decapping scavenger enzyme DCPS [1]. In the current study we asked whether that link holds in primary AML samples, how common FHIT-low disease may be across AML cohorts, whether myelodysplastic syndrome (MDS) also fits within this biomarker framework, and whether a more clinically accessible proxy biomarker could be found. The core finding was both encouraging and cautionary: low FHIT expression did predict sensitivity to the DCPS inhibitor RG3039, but hydroxyurea pretreatment confounded that signal in primary AML samples by reducing their sensitivity to treatment. At the same time, the broader cohort analyses showed that FHIT-low biology is relevant in a meaningful subset of disease, including 5–24% of AML, with the highest prevalence reported in pediatric AML (24.4%). FHIT promoter methylation was present in 35.8% of MDS and, notably, remained stable during azacitidine treatment, suggesting that FHIT-low predictive value may be feasible beyond AML. Most importantly, IDH2 mutation status emerged as a clinically accessible proxy biomarker for FHIT-linked DCPS sensitivity in AML [2].
That shift, from an interesting biomarker to a usable one, is really the story behind the paper. Biomarkers matter in oncology because they can reduce biological heterogeneity that can hide a real treatment effect in a clinical study. The numbers back this up: one large analysis of oncology drug-development programs found that biomarker-selected trials succeeded at roughly seven times the rate of unselected ones (10.7% versus 1.6%) [3]. A separate large-scale analysis across several major cancer types reported a nearly fivefold higher likelihood of approval when biomarkers were used [4]. These studies are retrospective rather than predictive for any single program, but they make a clear case for why biomarker-guided drug development has become so central in oncology.
However, a biomarker is only helpful if it can be used prospectively. That is where many promising ideas stall. A novel marker may be biologically compelling but practically difficult because it requires a specialized assay, an impractical measurement, or a workflow that most diagnostic labs simply do not run. The FDA’s enrichment guidance puts it plainly: to use a predictive biomarker to select patients who are more likely to respond to treatment, that marker has to work reliably enough to tell responders from nonresponders in a clinical setting [5].
This is where proxy biomarkers become valuable. They do not replace the underlying biology; they provide a more practical way in. FHIT remains the informative signal, but IDH2 mutation offers a cleaner clinical handle because it is already part of routine diagnostic testing. That means easier screening, tighter eligibility, and robust patient selection across multiple sites. In other words, the scientific question stays the same, but the path to testing it becomes less complicated.
This logic also affects trial design and cost. The FDA frames predictive enrichment as a way to improve efficiency by focusing on patients most likely to respond, which means a smaller study can still detect a real treatment effect. The math is striking: if only 25% of patients carry the relevant marker and the rest are unlikely to benefit, an unenriched trial may need up to 16 times more patients than an enriched one [5]. In practice, that translates to fewer patients to screen, fewer sites, faster recruitment, and much cheaper path to a proof-of-concept outcome.
For us, this is what made this paper satisfying. It started with a mechanistic biomarker hypothesis around FHIT and became a much more practical question: how do you carry elegant biology into a real clinical trial? Not by stepping away from the science, but by building a bridge between biology and deployment. IDH2 is that bridge: not a replacement for FHIT, but a clinically actionable way to reach it. In oncology drug development, this is the kind of bridge that often separates an interesting finding from a strategy that can be actually tested.
References
- Grassi F, Singh M, Moussaud S, Vazquez Rodruguez G, Ali Z, et al. DCPS is a synthetic lethal therapeutic target in acute myeloid leukemia expressing low levels of FHIT. Leukemia39, 2021–2025 (2025). DOI: 10.1038/s41375-025-02661-z
- Grassi F, Bast L, Singh M, Tobiasson M, Walfridsson J, de Milito A, et al. Integrated FHIT and IDH2 biomarker profiling predicts lethal sensitivity to DCPS inhibition in Acute Myeloid Leukemia and Myelodysplastic syndrome. Discover Oncology. 2026. DOI: 10.1007/s12672-026-04880-x
- Wong CH, Siah KW, Lo AW. Estimation of clinical trial success rates and related parameters. Biostatistics. 2019;20(2):273–286. DOI: 10.1093/biostatistics/kxx069
- Parker JL, et al. Does biomarker use in oncology improve clinical trial failure risk? A large-scale analysis. Cancer Medicine. 2021;10(6):1955–1963. DOI: 10.1002/cam4.3732
- U.S. Food and Drug Administration. Enrichment Strategies for Clinical Trials to Support Determination of Effectiveness of Human Drugs and Biological Products. Guidance for Industry. March 2019. Official FDA guidance (PDF)
Follow the Topic
-
Discover Oncology
This is a fully open access general oncology journal that aims to provide a unified forum for researchers and clinicians. The journal spans from basic and translational science, to preclinical, clinical, and epidemiology, and welcomes content that interfaces at all levels of cancer research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Prostate Cancer - Advances in Diagnosis and Treatment
Prostate cancer remains one of the most prevalent malignancies among men globally, accounting for a significant proportion of cancer-related morbidity and mortality. With increasing life expectancy and improved diagnostic techniques, the incidence and detection rates of prostate cancer continue to rise, highlighting the critical need for advances in both diagnostic and therapeutic approaches. Recent breakthroughs in molecular biology, imaging technologies, and genetic profiling have significantly enhanced early detection and prognostic accuracy, allowing for more personalized patient care.
This Collection aims to present comprehensive insights into recent developments and cutting-edge research in prostate cancer diagnosis and treatment. Key topics include novel biomarkers for early detection, advances in imaging modalities such as multiparametric MRI and PET-PSMA, genomic and epigenetic factors influencing disease progression, and emerging therapeutic strategies including robotic-assisted surgery, radiotherapy advancements, immunotherapy, and precision medicine approaches. Additionally, the collection will explore mechanisms of resistance to therapy, the role of tumor microenvironment in disease evolution, and strategies to overcome treatment barriers. We invite contributions focusing on translational and clinical research, innovative diagnostic methods, therapeutic innovations, and studies that bridge fundamental discoveries with clinical application to improve patient outcomes in prostate cancer.
Keywords: prostate cancer, biomarkers, imaging, genomics, precision medicine, robotic surgery, radiotherapy, immunotherapy, tumor microenvironment
Publishing Model: Open Access
Deadline: Jan 04, 2027
The Evolving Landscape of Lung Cancer: Advances in Diagnosis, Treatment Strategies, and Simultaneous Care
Lung cancer remains one of the leading causes of cancer-related mortality worldwide, although recent years have seen remarkable progress in its clinical management. This Collection aims to deepen the evolving landscape of lung cancer through a comprehensive lens, including early diagnosis, molecular profiling (through liquid and tissue), therapeutic innovation, and simultaneous care strategies. The Collection will gather original research, reviews, short reports or letters and case studies focused on:
advances in early detection and biomarker discovery and development;
the evolution of precision oncology and molecular profiling;
updates on systemic therapies, including immunotherapy and targeted agents;
novel treatment combination strategies,
the increasing integration of simultaneous care into multidisciplinary models for improving patient outcomes.
Keywords: lung cancer; precision oncology; immunotherapy; molecular diagnostics; simultaneous care
Publishing Model: Open Access
Deadline: Dec 04, 2026
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in