The allocation of preventive interventions: the case of COVID-19 vaccination schedules
Published in Social Sciences


In the early stage of the COVID-19 pandemic, many professional associations, healthcare institutions, and governmental bodies published or updated prioritization guidelines regarding the allocation of scarce medical resources, e.g., beds or artificial ventilation in intensive care units. Later, in the second half of 2020, many governments published detailed prioritization schedules for the distribution of COVID-19 vaccines, which were scarce goods at the turn of 2020 and 2021. Unlike guidelines on medical treatment (Hans‐Jörg et al., 2021), official schedules on the distribution of medical prevention have not yet been analyzed or compared in scholarly journals. Thus, our main aim is to provide the first systematic international comparison of the official prioritization schedules for vaccinations in 29 countries (EU, UK, and Israel) and to analyze the values and principles implicitly embedded in these documents. Although some scholars suggest that prioritization during the pandemic raises structurally similar dilemmas in the cases of diagnosis, treatment, and prevention (Emanuel et al. 2020), we highlight and analyze the specific nature of allocation decisions in the case of prevention.
Our study shows that two groups were vaccinated first in almost all of the researched countries: frontline medical workers as well as personnel and residents of nursing homes. We assume that the reasons why they were prioritized are mixed: direct (protecting persons belonging to this group) and indirect (because of someone else’s interests).
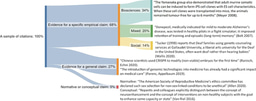
To interpret other value choices embedded in the analyzed schedules, we differentiated between two main types of direct priority categories: groups that have an increased infection fatality rate (IFR) compared to the average for the general population and groups chosen because their members experience an increased risk of being infected (ROI). We also distinguished two subcategories in each category. Increased IFR stems from an individual's physical state: suffering from certain health conditions or just being of an older age. Increased ROI is mainly determined by factors related to measurable social mobility - an increased number of social contacts compared to average in the population. Thus, we distinguished between two factors: working and housing conditions.
Each analyzed country emphasized prioritizing senior members of society (either dividing them into a few fine-grained cohorts or treating those above some age threshold as one group), and some schedules prioritized people almost entirely based on their IFR – this is the case of the UK. On the other side of the spectrum were countries that additionally used many other factors that we interpreted as targeting people with increased ROI – this was the case of Germany (see Figure 1).

Then, we discuss how the comparison of COVID-19 vaccine schedules may be helpful in interpreting the different value choices regarding priority-setting in prevention. In particular, we are interested in how three groups of principles (utilitarian, prioritarian, egalitarian) commonly treated as relevant in the healthcare contexts were embedded in the vaccine schedules.
First, the utilitarian approach promises to provide a straightforward solution to the allocation of healthcare resources by calculating and weighing the benefits (e.g., numbers of lives saved, years of life saved, quality-adjusted life-years saved) in a quantifiable manner. In fact, in most guidelines regarding treatment (e.g., ventilators in the case of COVID-19), it is not only saving lives that is considered and prioritized, but also a variety of other factors, particularly the probability of short-term survival as well as long-term considerations such as life expectancy and the quality of future life. In contrast, in the case of COVID-19 vaccination schedules, the vast majority of groups with prioritized access to vaccination were included mainly based on their uncertain and narrowly understood prospects related to COVID-19 infection: as one may interpret, the worse their prospects were in this matter and the more probable that they may die because of COVID-19, the higher on the vaccination priority list they found themselves. The concentration on IFR, particularly in age cohorts, visible in the analyzed schedules has a pragmatic justification based on the asymmetry of evidence. In the case of COVID-19, including someone in a high-risk group may have a different meaning. On the one hand, it may be based purely on medical premises (IFR); on the other hand, it may be primarily social-based (ROI). We hypothesize that this aspect is particularly interesting while analyzing utilitarian principles: schedules implement principles that depend on such social factors to a lesser extent because it is much more difficult to predict the results of their implementation.
Second, many of the discussions about prioritarianism in healthcare assume that a decision-maker should categorize the worst off by referring either only (or primarily) to their entire lifespan (like a life-time prioritarianism) or only (or mostly) to some part of their lifespan (like a time-slice prioritarianism). This distinction is visible in the well-known distinction between 'youngest first' and 'sickest first' versions of prioritarianism (Persad et al. 2009). However, neither of these understandings of the worst off can be applied to interpret the COVID-19 vaccine distribution schedules, which strongly prioritized older persons and took into account mainly patients’ prospects (but not their current or past health conditions). The fact that ROI-based criteria were not systematically and consistently applied may be interpreted as implementing the principle that the worst off are those who have the highest risk of death if infected, that is, the highest IFR.
Third, our analysis shows that the egalitarian principle was only adopted in the analyzed vaccination schemes in a limited form. The egalitarian approach serves there exclusively as a second-order principle, namely, as a pattern of distribution within already prioritized groups (that is, groups which are distinguished on the basis of some other criteria). In particular, the “first come, first serve” approach was to distribute vaccines within subsequent groups. Furthermore, and particularly noteworthy, no researched priority setting adopted a chancy mechanism to distribute COVID-19 vaccines – either in the version of an identical chance lottery or a weighted lottery. This may suggest that random distribution, which is often discussed by philosophers, has, in fact, limited practical applications in the prioritization of healthcare prevention.
Finally, we investigate how to interpret the observed patterns of prioritization in COVID-19 vaccination schedules. Do they stem from some systematic differences between curative and preventive medical interventions that may influence the prioritization rules? For example, from the fact that prioritization in the case of preventive interventions always concerns merely statistical individuals? Or from the intricacy of ascribing causal claims to the case of preventive medical interventions, which may be understood as a matter of causing the non-occurrence of an event? Surprisingly, in contrast with many medical treatments (e.g., the allocation of organs for transplantation), there is no well-established expert consensus on the allocation of preventive interventions.
We conclude that the theoretical ambiguity of vaccine distribution patterns might paradoxically be regarded as an advantage in political practice. The legitimization criteria applied by bioethical experts and the general public typically differ, whereas social legitimacy, which is crucial for the effectiveness of vaccine policies, is mainly dependent on the latter. The tension between bioethics experts and public opinion was clearly visible in the case of the allocation of respirators in the first phase of COVID-19 in the US, where the decision not to give the respirator to disabled people or people suffering from certain diseases, albeit motivated by the basis of well-considered bioethical reasoning, aroused protests and in some cases led to changes in the guidelines (Orfali 2021). In contrast, the fact that established schedules could be interpreted and defended on different normative grounds may increase their legitimacy in the eyes of the public.
Acknowledgments
This summary is partially based on Wiśniowska, Żuradzki, & Ciszewski (2022). This research was supported by the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement 805498).
References
Emanuel, E.J., Persad, G., Upshur, R. et al. (2020), Fair allocation of scarce medical resources in the time of Covid-19. New England Journal of Medicine 382(21), 2049-2055. DOI: https://www.nejm.org/doi/10.1056/NEJMsb2005114
Hans‐Jörg, E., Wiesing, U., & Ranisch R. (2021). Saving the most lives—A comparison of European triage guidelines in the context of the COVID‐19 pandemic. Bioethics 35(2),125-134. DOI: https://doi.org/10.1111/bioe.12836
Giubilini, A., Savulescu, J., & Wilkinson, D. (2021). Queue questions: Ethics of COVID‐19 vaccine prioritization. Bioethics 35(4),348-355. DOI: https://doi.org/10.1111/bioe.12858
Orfali, K. (2021). Getting to the Truth: Ethics, Trust, and Triage in the United States versus Europe during the Covid‐19 Pandemic. Hastings Center Report 51(1),15-22. DOI: https://doi.org/10.1002/hast.1206
Persad, G., Wertheimer, A., & Emanuel, E.J. (2009). Principles for allocation of scarce medical interventions. The Lancet 373 (9661),423-431. DOI: https://doi.org/10.1016/S0140-6736(09)60137-9
Schmidt, H., Weintraub, R., Williams, M.A. et al. (2021). Equitable allocation of COVID19 vaccines in the United States. Nature Medicine 27,298–307. DOI: https://doi.org/10.1038/s41591-021-01379-6
Wiśniowska, K., Żuradzki, T., & Ciszewski, W. (2022). Value choices in European COVID-19 vaccination schedules: How vaccination prioritization differs from other forms of priority-setting. Journal of Law and the Biosciences. Volume 9, Issue 2, July-December 2022, lsac026, DOI: https://doi.org/10.1093/jlb/lsac026
I'm an associate professor at the Institute of Philosophy at Jagiellonian University in Kraków (Poland) and the director of the Interdisciplinary Centre for Ethics at Jagiellonian University. I currently lead the project BIOUNCERTAINTY funded by the European Research Council (ERC) Starting Grant. My work focuses on various topics at the intersection of metaethics, practical ethics, and philosophical bioethics.
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in