What Does Evidence-Based Mentalization Therapy Look Like in Practice?
Published in Behavioural Sciences & Psychology
Mentalization has become one of the central concepts in contemporary psychotherapy, attachment research, and developmental psychology. The term refers to the capacity to form mental representations of intentional mental states — such as emotions, needs, desires, beliefs, and purposes — and thereby to understand these states in oneself and others. In recent decades, Mentalization-Based Therapy (MBT), developed by Peter Fonagy and Anthony Bateman, has emerged as an evidence-based treatment approach specifically aimed at strengthening this capacity.
Yet despite the growing popularity of the concept, one important question often remains surprisingly unclear: what does mentalization actually look like in clinical practice? Many clinicians may understand the concept theoretically while still lacking a vivid picture of how mentalizing is restored within actual therapeutic dialogue.
Our article, Making Visible the Clinical Practice of Mentalization-Based Therapy as Illustrated by Therapy Session Material, was written to clarify these questions in a concrete and educational manner. The background to the article was itself deeply dialogical. During the autumn of 2024, we began a series of conversations about mentalization and related concepts from two different professional perspectives. One of us approached the topic primarily as a doctoral researcher interested in conceptual clarity and theory development; the other as a practicing psychotherapist with years of direct clinical experience. Very quickly, we noticed that achieving a shared understanding of mentalization required far more than simply reviewing theoretical definitions.
This realization led us to examine an actual MBT session example in detail, and our dialogue gradually evolved into the idea of presenting our shared reflections in the form of an article.
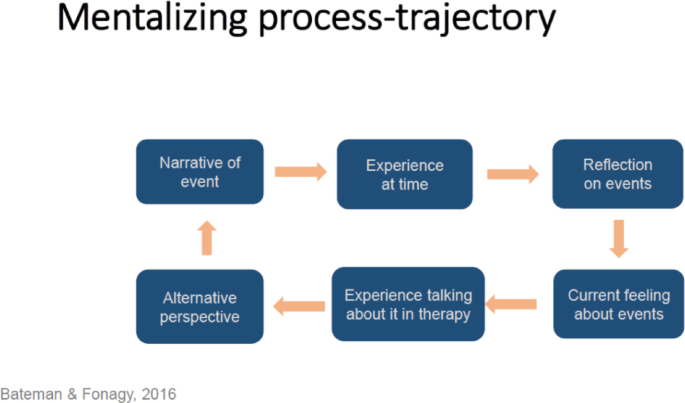
The therapy example we analyze centers on a fictional patient, Susan, whose therapist unexpectedly had to cancel a session while she is already on her way to the appointment. What initially appears to be a relatively minor event gradually reveals itself to be emotionally overwhelming for the patient. Following the cancellation, Susan experiences intense distress and eventually induces vomiting. At first, however, she is unable to describe clearly what she felt. Her experience appears only as a vague “bad feeling” rather than as a differentiated emotional state connected to a meaningful relationship.
Our article describes how MBT helps transform such unmentalized emotional states into experiences that can gradually be recognized, reflected upon, and shared. The therapist does not impose interpretations from outside or claim to know the patient’s mind. Instead, the therapist adopts what MBT describes as a mentalizing stance: a curious, exploratory, and not-knowing attitude that repeatedly invites the patient to examine experience more closely.
When the therapist’s understanding feels sufficiently accurate and emotionally attuned, it strengthens the patient’s epistemic trust: the capacity to receive and internalize personally meaningful information from another person. In the session example, the gradual restoration of mentalizing ultimately leads to a shared relational state described as we-ness — a moment of mutual understanding in which both therapist and patient experience emotional connection and shared meaning.
We also aim to discuss how the mentalization-based approach relates to other forms of psychotherapy. MBT proposes that mentalizing is restored and strengthened primarily within the therapeutic relationship itself. What distinguishes the approach, however, is its particular focus on moments of rupture and repair, and on the careful working through of these moments in accordance with MBT principles. MBT focuses on helping the patient regain the capacity to reflect on feelings, intentions, and relationships while consistently working within the patient’s zone of proximal development.
In many ways, the process through which we wrote the article mirrored the very principles we were describing. The text itself emerged through dialogue, mutual questioning, clarification, and the gradual development of shared understanding. In this sense, the writing process itself reflected what mentalizing fundamentally is: a deeply human process through which people create meaning together.
By closely examining a single therapy interaction, we hope to offer psychotherapists, researchers, and students a clearer understanding of how mentalization can be supported, restored, and stabilized in therapeutic work. Making the mechanisms of action in MBT visible is important for all therapists interested in the role of mentalizing in psychotherapy. Psychotherapists interested in this approach may compare the mentalizing approach presented here with their own clinical way of working.
Follow the Topic
-
Discover Mental Health
This is an international, open access journal that publishes research across the transdisciplinary field of mental health research.

Related Collections
With Collections, you can get published faster and increase your visibility.
Mental Health Inequities and Disparities: Behavioral Pathways, Intervention Targets, and Global Policy Implications
This collection seeks to advance understanding of mental health inequities by explicitly focusing on behavioral pathways that link structural, social, and economic inequities to mental health outcomes. Rather than addressing social determinants in broad terms, the Collection emphasizes how inequities rooted in socioeconomic status, race and ethnicity, gender, geography, and disability shape health-related behaviors (e.g., substance use, diet, physical activity, sleep, and help-seeking), and how these behaviors constitute modifiable targets for intervention, service design, and policy action.
Health inequities are systematic, avoidable, and unjust differences in health that both contribute to and result from mental health problems. These inequities often operate through behavioral and psychosocial mechanisms that exacerbate mental and physical health disparities across the life course. The Collection welcomes large-scale epidemiological and cohort studies, registry-based analyses, qualitative and mixed-methods research with marginalized populations, implementation and dissemination studies, natural experiments and policy evaluations, as well as digital, community-based, and behavioral interventions grounded in behavioral science and health psychology.
By integrating perspectives from public health, epidemiology, behavioral science, health psychology, and intervention research, this interdisciplinary Collection aims to generate evidence that is directly relevant for translating research into policies and practices that promote mental health equity in diverse global contexts.
Keywords:
Mental health disparities; Health inequities; Social determinants of mental health; Health behavior; Structural inequity; Psychosocial stress; Health equity interventions; Global mental health; Socioeconomic status; SDG 3 (Good Health and Well-being); Behavioral science; Health psychology; Behavioral interventions; Policy translation
Publishing Model: Open Access
Deadline: Oct 21, 2026
Child and Adolescent Mental Health: Challenges and Innovations
Child and adolescent mental health is an urgent global concern, with increasing prevalence of anxiety, depression, behavioral problems, neurodevelopmental disorders, and self-harm. Rapid social changes, academic pressures, digital and social media influences, and the lingering psychological impacts of the COVID-19 pandemic have intensified vulnerabilities in this age group. Persistent gaps remain in early detection, equitable access to care, interdisciplinary collaboration, and the safe integration of evidence-based innovations into clinical and community settings.
This Collection aims to provide a comprehensive platform for emerging research, critical reviews, and practice-based insights that advance understanding of mental health challenges among children and adolescents—while highlighting transformative innovations. We especially welcome studies on digital health and artificial intelligence (AI), including AI-assisted screening, machine learning–driven predictive models, tele-mental health, virtual reality therapies, and mobile applications designed for youth and families.
Recognizing that digital and AI-driven approaches carry unique risks for young populations, this Collection places strong and explicit emphasis on addressing the ethical, access, and data-privacy challenges embedded in these technologies. We actively encourage submissions that explore:
• Ethical safeguards and governance models for responsible AI use in youth mental health, including algorithmic transparency, bias mitigation, informed consent, and child-safeguarding principles;
• Data-privacy and security frameworks that protect sensitive behavioral, emotional, and biometric data collected through digital platforms;
• Equitable access challenges, including digital divides, disparities in device/internet availability, structural inequities, and cultural or linguistic barriers that limit benefit from digital innovations;
• Evaluation of risks, such as data misuse, surveillance, stigmatization, or unintended harms resulting from automated decision-making;
• Policy, regulatory, and implementation guidelines that ensure digital and AI tools are safe, trustworthy, and centered on the rights and well-being of children and adolescents.
By elevating these critical concerns, the Collection seeks to promote innovations that are not only technologically advanced but also ethically responsible, privacy-protective, culturally sensitive, and accessible across diverse global contexts.
In addition to digital innovations, the Collection welcomes scholarship on school-based programs, family-centered care, trauma-informed interventions, and community-level strategies. Bringing together perspectives from nursing, psychiatry, psychology, public health, data science, social sciences, and education, this Collection aims to stimulate global dialogue, strengthen evidence-based practice, and support the development of safe, scalable, and person-centered mental health solutions. Ultimately, the goal is to enhance resilience, reduce stigma, expand equitable access to quality care, and shape the future of child and adolescent mental health worldwide.
Keywords:
• Child mental health
• adolescent mental health
• Pediatric psychiatry
• cytogenetics
• neurodevelopmental Disorders
• Behavioral disorders
• Anxiety and depression
• Self-harm and suicide prevention
• Early identification and prevention
• Community-based mental health care
• Mental health nursing
• Artificial intelligence in mental health
• Tele-mental health
• mHealth applications
• Virtual reality–based interventions
• Ethical AI in youth mental health
Publishing Model: Open Access
Deadline: Aug 31, 2026


Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in