What We Get Wrong About “What Works for Whom” in Childhood Anxiety
Published in Behavioural Sciences & Psychology

Why this research mattered to me
One of the first questions I heard as a student was: “Which treatment is best for this child?” And despite decades of research, we still don’t have a confident answer.
Realising that treatment responses differ between children, and that “moderation” is the tool we use to study this, I dived into the chaos. I wanted to understand what was really happening behind all those moderator analyses scattered across the literature. Were we actually close to identifying who benefits most from CBT? Or were we stuck in a loop of inconsistent terminology, poor reporting, and methodological mismatches?
Spoiler: mostly the second thing.
How the project unfolded (and what surprised us)
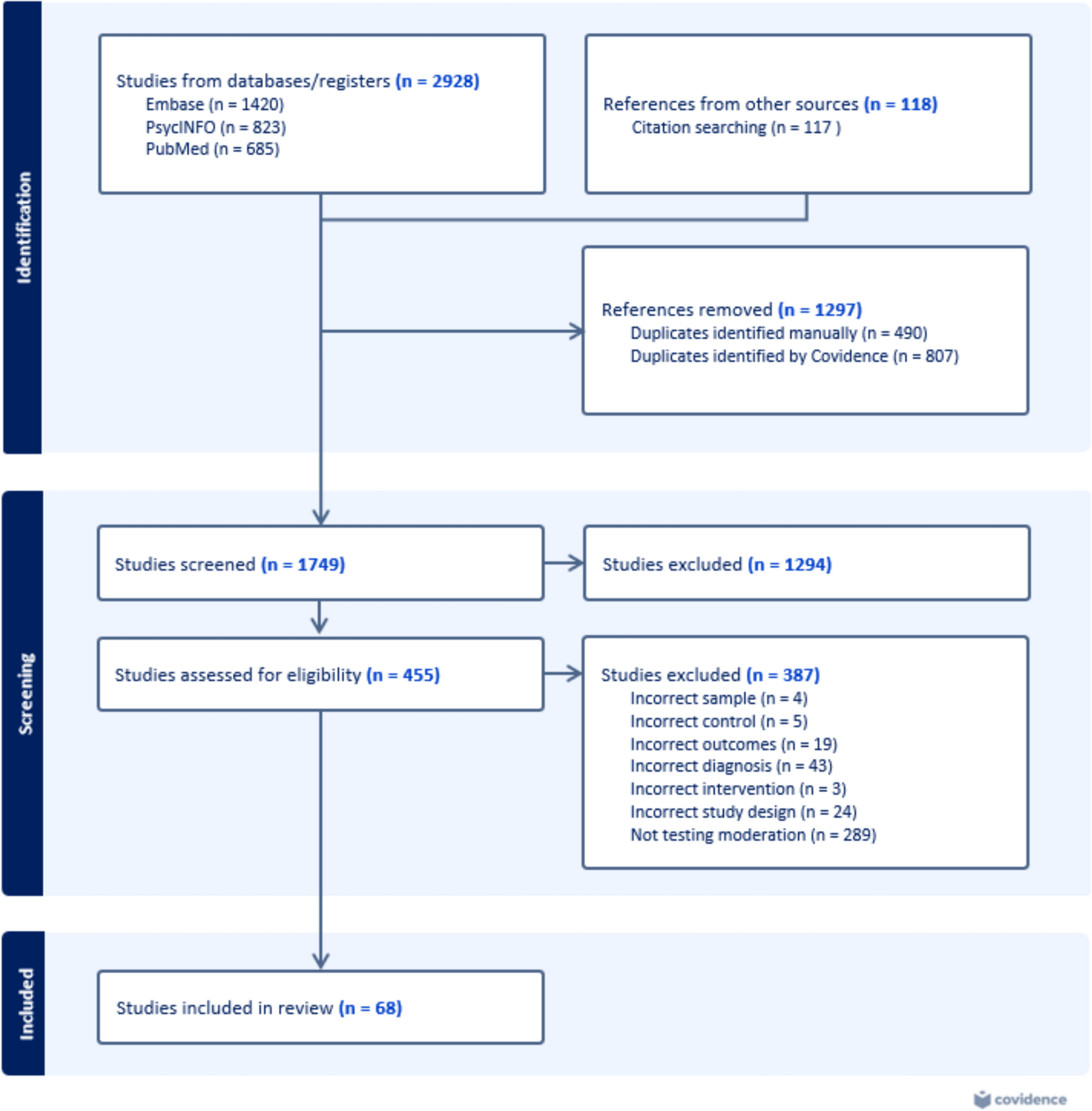
This project began with a naïvely ambitious belief that we would “quickly” synthesise moderator evidence. The deeper we went, the clearer it became that almost no two studies were speaking the same language. Our final search delivered 68 studies from 44 trials, each offering a piece of the puzzle.
Despite the heterogeneity, we mapped everything: demographic factors, clinical characteristics, family context, treatment processes, and even biological markers. When we laid the studies side by side, the same problems kept reappearing:
- Variables labelled as “moderators” without clear definitions
- post‑baseline characteristics treated as predictors of differential treatment response
- inconsistent control conditions
- interactions tested for convenience rather than theory
- underpowered analyses interpreted as meaningful
- outcomes measured at different times, in different ways
Even so, we did find patterns, just not the tidy ones the field keeps hoping for. Moderator variables like age, social anxiety diagnosis, baseline severity, parent psychopathology, and parent acculturation showed hints of consistent differential effects. But none met our strict criteria for being robust, that is, consistently defined, adequately powered, and replicated across trials.
Instead of a clear “treatment matching” map, what emerged was a story of a field trying to do the right thing with tools that weren’t built for the job. Despite the complexity, our overarching aim remained the same: to strengthen the evidence clinicians rely on for treatment planning, to offer families clearer guidance about what may work best for their child, and to move beyond one-size-fits-all approaches for young people.
So, what does this mean for the future of personalised care?
To move forward, we’ll need:
- Shared language and strict definitions: “Moderator” shouldn’t mean different things. We need conceptual clarity before methodological precision is possible.
- Better-designed trials and pre-registered hypotheses: Too many moderation tests are exploratory or underpowered. Without clear intentions, findings become noise rather than signals.
- Comparable outcome measures and aligned control conditions: We can’t build cumulative knowledge when everyone measures improvement differently.
- Larger datasets and modern analytic tools: Moderator effects are small. Individual patient data meta-analyses, pooling RCT datasets, and machine learning aren’t luxuries; they’re increasingly essential.
- A shift from ‘finding the one magic variable’ to capturing the complexity of real children: Single moderators rarely hold the key. Combinations of factors likely matter more.
Looking back, and ahead
What started as “just a review” turned into a sweeping audit of how an entire field studies heterogeneity. By the time we completed the study in 2025, I understood why progress has been slow, but also why the future is promising.
This paper doesn’t declare that personalisation is impossible. Quite the opposite. It offers the foundation the field needs: clarity about the gaps, a roadmap for change, and a call to collaborate rather than accumulate mismatched studies.
For researchers, I hope it encourages more careful, collaborative approaches to studying heterogeneity. For clinicians and families, I hope it reassures them that the question they ask most often is the right one, even if the science is still catching up.
Follow the Topic
-
Clinical Child and Family Psychology Review
This is an international, interdisciplinary forum for identifying new developments and reviewing current thought and practices in the broad area of the behavioral sciences that pertains to infants, children, adolescents, and families.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in