When Psychiatry Is Not Primary: A Rare Prion Disease Unmasked
Published in Neuroscience and Biomedical Research
Case Overview
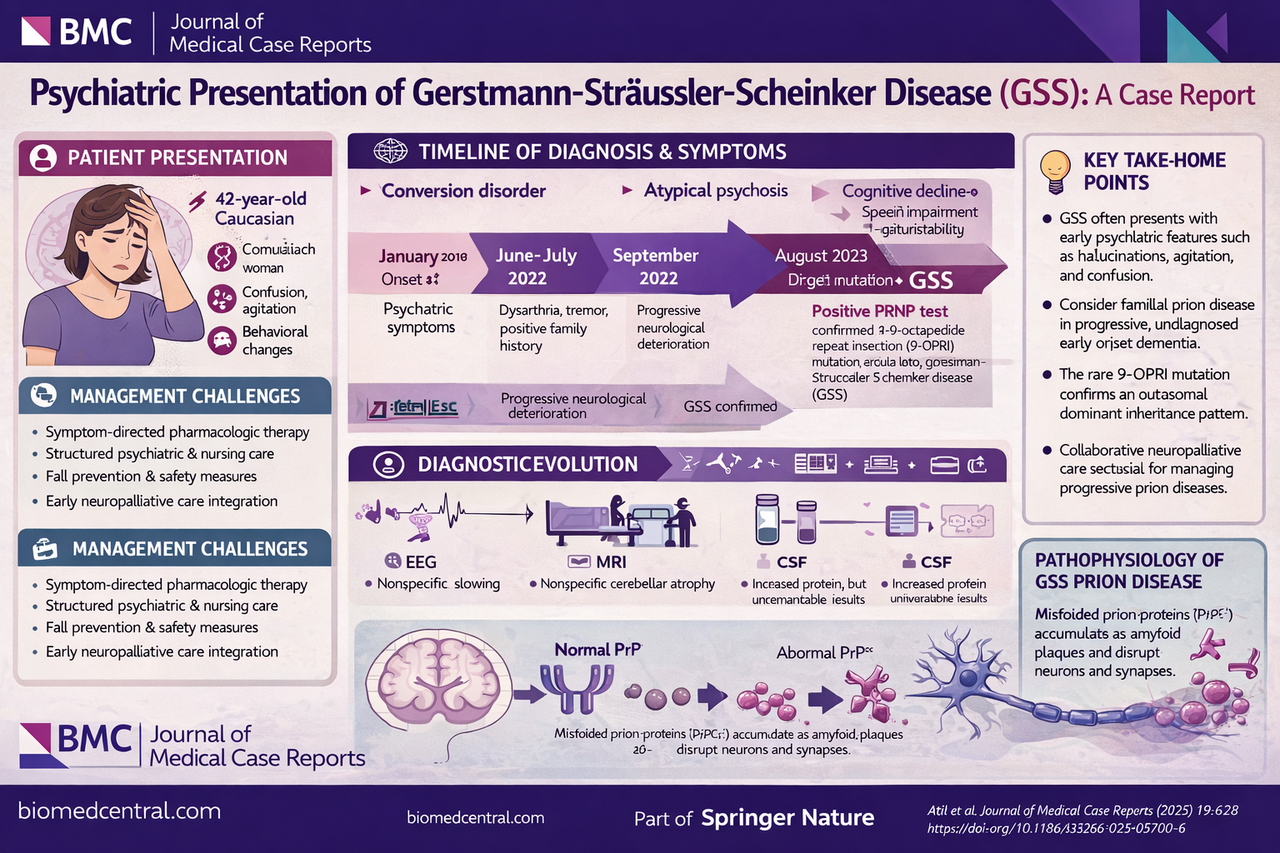
A 42-year-old woman presented with progressive confusion, agitation, insomnia, and behavioral disturbances, ultimately requiring psychiatric hospitalization. Early symptoms included tremor, dysarthria, and psychomotor slowing, which were initially attributed to conversion disorder.
Over time, the clinical picture evolved to include:
Progressive cognitive decline
Gait instability and recurrent falls
Dysarthria and impaired communication
Emotional lability and severe sleep disturbance
A key turning point was recognition of a positive family history, prompting genetic testing. This confirmed a 9-octapeptide repeat insertion (9-OPRI) mutation in the PRNP gene, establishing the diagnosis of GSS .
Why This Case Matters
This case underscores several critical clinical principles:
Psychiatric-first presentations are common in prion disease—reported in up to 87% of cases
Misdiagnosis is frequent, particularly as functional or primary psychiatric disorders
Standard neurodiagnostics (MRI, EEG, CSF) may be nondiagnostic early
Family history remains pivotal in triggering appropriate genetic evaluation
Notably, the 9-OPRI mutation is exceptionally rare, with only a handful of reported cases worldwide .
Management Challenges
There is no disease-modifying therapy for GSS. Management is therefore centered on:
Symptom-directed pharmacologic therapy (e.g., antipsychotics, antidepressants, sleep agents)
Structured psychiatric and nursing care
Fall prevention and environmental adaptation
Early integration of neuropalliative care
This case also highlights the substantial caregiver burden, requiring coordinated multidisciplinary support.
Clinical Pearl
In younger patients with atypical psychiatric syndromes—especially with progressive neurological features or family history—consider prion disease and pursue genetic testing earlier.
Question
Which feature should most strongly prompt reconsideration of a primary psychiatric diagnosis in this context?
A. Acute onset insomnia
B. Emotional lability
C. Progressive neurological decline with family history
D. Response to antipsychotics
Answer: C
The combination of progressive neurological deterioration and a positive family history is a red flag for underlying neurodegenerative or genetic disease, warranting targeted testing such as PRNP analysis.
Closing Perspective
This case is a powerful reminder that not all psychiatric presentations are psychiatric in origin. As neurologists and clinicians, maintaining diagnostic vigilance—particularly in atypical, progressive, or familial cases—remains essential.
Rare diseases such as GSS, while uncommon, offer profound insights into neurodegeneration, diagnostic reasoning, and the importance of integrated neurologic and psychiatric care.
Journal of Medical Case Reports is the world’s first international, PubMed-listed, medical journal devoted to publishing case reports from all medical disciplines and will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.
Richard Alan Rison is the interim Editor-in-Chief of Journal of Medical Case reports. He is also an associate neurology editor (editorial board) for BMC Neurology, and the former lead editor for case reports of BMC Research Notes (currently on the editorial board). His scholarly work focuses on medical case reporting, reporting standards, and editorial methodology. Dr. Rison participated in the development and dissemination of the CARE guidelines for clinical case reporting and has authored numerous publications addressing both neurological disorders and the role of case reports in advancing medical knowledge. Dr. Rison practices general neurology and served as the founding medical director of the PIH Health Hospital-Whittier Stroke Program and the PIH Health Hospital-Whittier Non-Invasive Vascular Laboratory, is a clinical assistant professor of neurology at the University of Southern California Keck School of Medicine and Los Angeles County Medical Center, and is a Fellow of the American Academy of Neurology, the American Neurological Association, and the American Association of Neuromuscular and Electrodiagnostic Medicine. Dr Rison is board-certified by the American Board of Psychiatry and Neurology in neurology and vascular neurology, and neurocritical care and neuroimaging by the United Council of Neurologic Subspecialties. He is also board-certified by the American Board of Electrodiagnostic Medicine in electrodiagnostic medicine. Dr. Rison is a former president of the Los Angeles Neurological Society.
Follow the Topic
-
Journal of Medical Case Reports
This journal will consider any original case report that expands the field of general medical knowledge, and original research relating to case reports.

Your space to connect: The Psychedelics Hub
A new Communities’ space to connect, collaborate, and explore research on Psychotherapy, Clinical Psychology, and Neuroscience!
Continue reading announcement
Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in