Behind the Paper: When Safety Becomes the MessageWhen Safety Becomes the Message
Published in Anatomy & Physiology
When I started performing thyroid thermal ablation, I was still a radiology resident. At that time, the field was in its infancy. The main challenge was not how to optimize the technique, but rather how to convince colleagues that it worked at all.
The early years were dedicated to demonstrating efficacy. Could we really reduce thyroid nodules without surgery? Could we offer patients a minimally invasive alternative that avoided scars, preserved thyroid function, and produced durable results? Equally important, could we prove that the procedure was safe?
Over the following years, together with many colleagues around the world, we generated evidence, published studies, developed guidelines, and worked tirelessly to introduce thyroid ablation into clinical practice. Gradually, what was once considered experimental became accepted. Today, thyroid thermal ablation is recognized internationally as an effective treatment option for selected patients with benign thyroid nodules.
Success, however, brought an unexpected challenge.
As the technique became more widespread, an increasing number of physicians became interested in performing it. This was encouraging, but it also revealed a potential problem. Because thyroid ablation is minimally invasive and is usually performed under local anesthesia, some practitioners began to perceive it as an easy procedure. Others, particularly those coming from backgrounds with limited experience in diagnostic ultrasound and ultrasound-guided interventions, started performing ablations without fully appreciating the complexity of image guidance.
For the first time in my career, I realized that demonstrating how safe a technique is may not be enough. Sometimes it is equally important to discuss when and why complications occur.
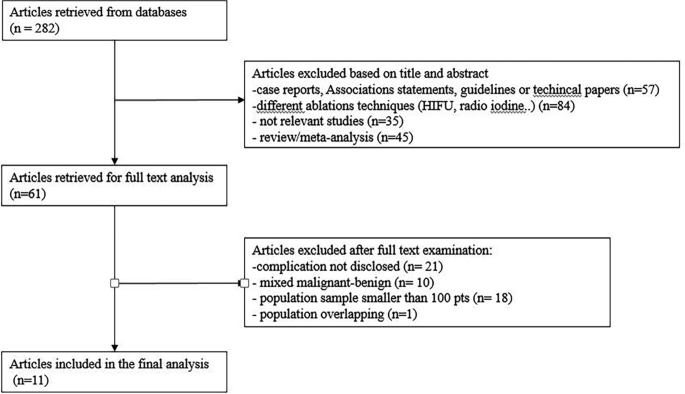
This realization was one of the main motivations behind our systematic review on complications of minimally invasive treatments for benign thyroid nodules. The literature consistently shows that thyroid ablation is a remarkably safe procedure, with major complications being exceedingly rare. Yet every complication tells a story. In many cases, complications are linked not to the technology itself, but to inadequate training, insufficient familiarity with neck anatomy, limited ultrasound expertise, or poor understanding of the physical principles governing thermal energy delivery.
The message of our review is therefore not that thyroid ablation is dangerous. Quite the opposite. The procedure has an excellent safety profile and has transformed the treatment of thyroid disease for thousands of patients worldwide. However, its safety depends on the operator.
Successful thyroid ablation requires much more than inserting a needle into a nodule. It requires a deep understanding of cervical anatomy, mastery of ultrasound imaging, experience with image-guided procedures, and the ability to recognize and prevent complications before they occur. These skills are acquired through dedicated training and mentorship, not simply by reading a protocol or purchasing a device.
Looking back, I find it interesting that my scientific journey has mirrored the evolution of the field itself. At the beginning, we had to prove that thyroid ablation worked. Today, we must ensure that it continues to work safely as its adoption expands worldwide.
In a way, this paper is not only about complications. It is about responsibility. The responsibility that comes with introducing a successful new technology into clinical practice and ensuring that its growth is accompanied by the same rigor, training, and attention to patient safety that allowed it to succeed in the first place.
Follow the Topic
-
La radiologia medica
This is a peer-reviewed journal intended as a medium for the communication of results and developments in the field of radiology, particularly on advances in diagnostic imaging and its allied sciences.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in